Palmoplantar keratoderma
Palmoplantar keratoderma
The palmoplantar keratodermas (PPKs) comprise a large heterogeneous group of acquired or inherited cornification disorders characterized by hyperkeratosis of the palms and soles.1 Hereditary PPK may be occur in
86 Disorders of keratinization
A
B
Palmoplantar keratoderma Disease Inheritance Gene
Diffuse Epidermolytic PPK Vörner-Unna-Thost, (including tonotubular subtype, epidermolytic hyperkeratosis with polycyclic psoriasiform plaques, progressive palmoplantar keratoderma Greither)
AD KRT1 or KRT9 Non-epidermolytic PPK, type Kimonis AD KRT1 type Bothnia AD AQP5 type Nagashima AR SERPINB7 Keratolytic winter erythema AD Unknown Mal de Meleda (including Gamborg-Nielsen) AR SLURP1
Circumscribed Striate palmoplantar keratoderma AD type 1 DSG1 type 2 DSP type 3 KRT1
Punctate Keratosis punctata palmoplantaris, AD type 1 (Buschke-Fischer-Brauer) AAGAB (COL14A1) type 2 (Spiny keratoderma) ? type 3 (Marginal papular acrokeratoderma) ?
isolation or associated with other genetic diseases, such as ichthyosis, erythrokeratoderma, epidermolysis bullosa, ectodermal dysplasia, and dyskeratosis congenita (Tables 3.6 and 3.7).2–6 When PPK is syndromic it may affect the heart, eyes, hearing or neural system. Acquired forms can be paraneoplastic or related to internal diseases. Therefore a specific diagnosis of PPK is mandatory for the purpose of management and genetic counseling.2
In many subtypes, the underlying molecular defect has been identified and can be related to structural proteins (keratins), cornified envelope (loricrin, transglutaminase), cohesion proteins (plakophilin, desmoplakin, desmoglein1), cell-to-cell communication (connexins, SLURP1, AAGAB), and epidermal proteases (cathepsin C).5,6,9
PKKs are classified on the basis of mode of inheritance, distribution of lesions, additional clinical features, and associated abnormalities.1–8 Many of the inherited forms of the PPK have a late onset and show variability in one and the same family. The severity also depends on mechanical stress, e.g., exposure to pressure on the feet. The patients may suffer from maceration, blisters, malodor, and/or severe pain. Hyperhidrosis and fungal infections are common complications.
There are three major clinical categories of inherited PPK: diffuse, circumscribed, and punctate (see Tables 3.6 and 3.7).4,7,8 Histologically, seven main histologic patterns have been proposed characterized by epidermolytic hyperkeratosis, orthohyperkeratosis or parakeratosis, hypergranulosis, transitional cells, widening of the intercellular spaces, intracytoplasmic eosinophilic inclusions, or depression of the epidermis with keratotic plaques (Table 3.8).
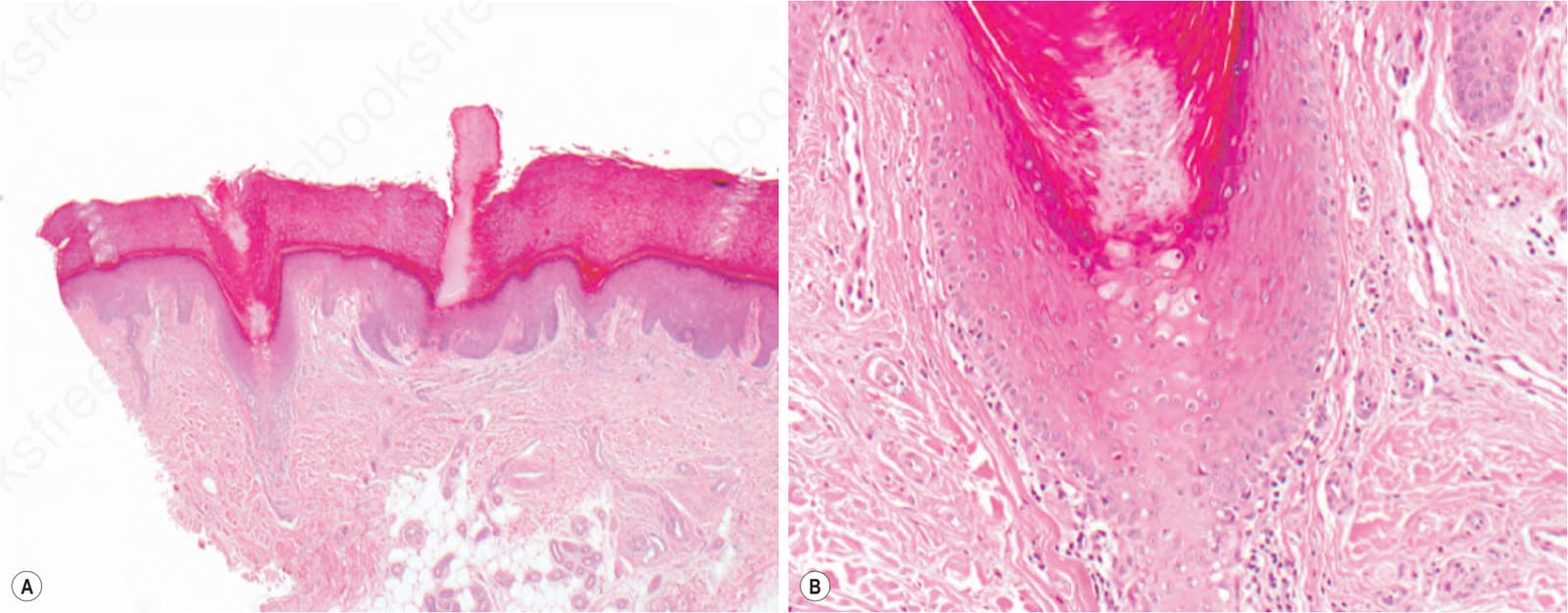
Fig. 3.81 Porokeratotic adnexal ostial nevus (PAON): (A) filiform keratoses, protrude from the dilated ostia of hyperplastic sweat glands and hair follicles; (B) the underlying epithelium reveals vacuolated epithelia with pyknotic nuclei and lacks keratohyalin granules.
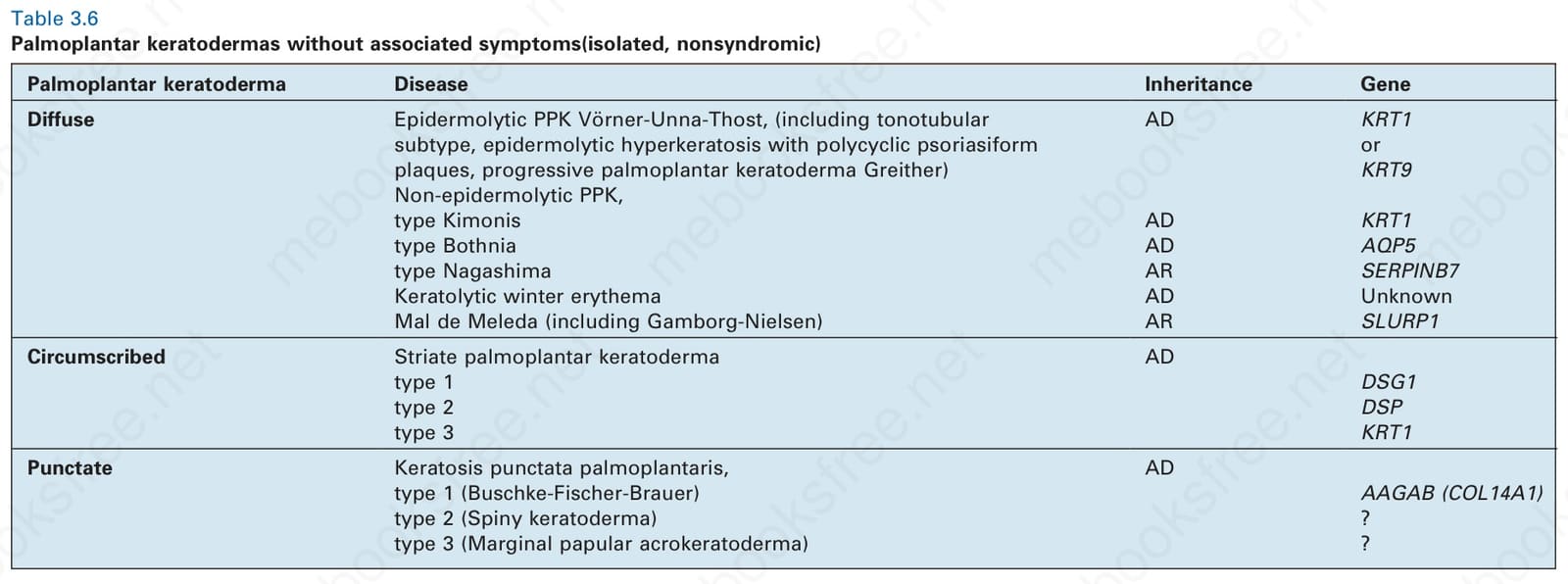
Table 3.6 Palmoplantar keratodermas without associated symptoms(isolated, nonsyndromic)
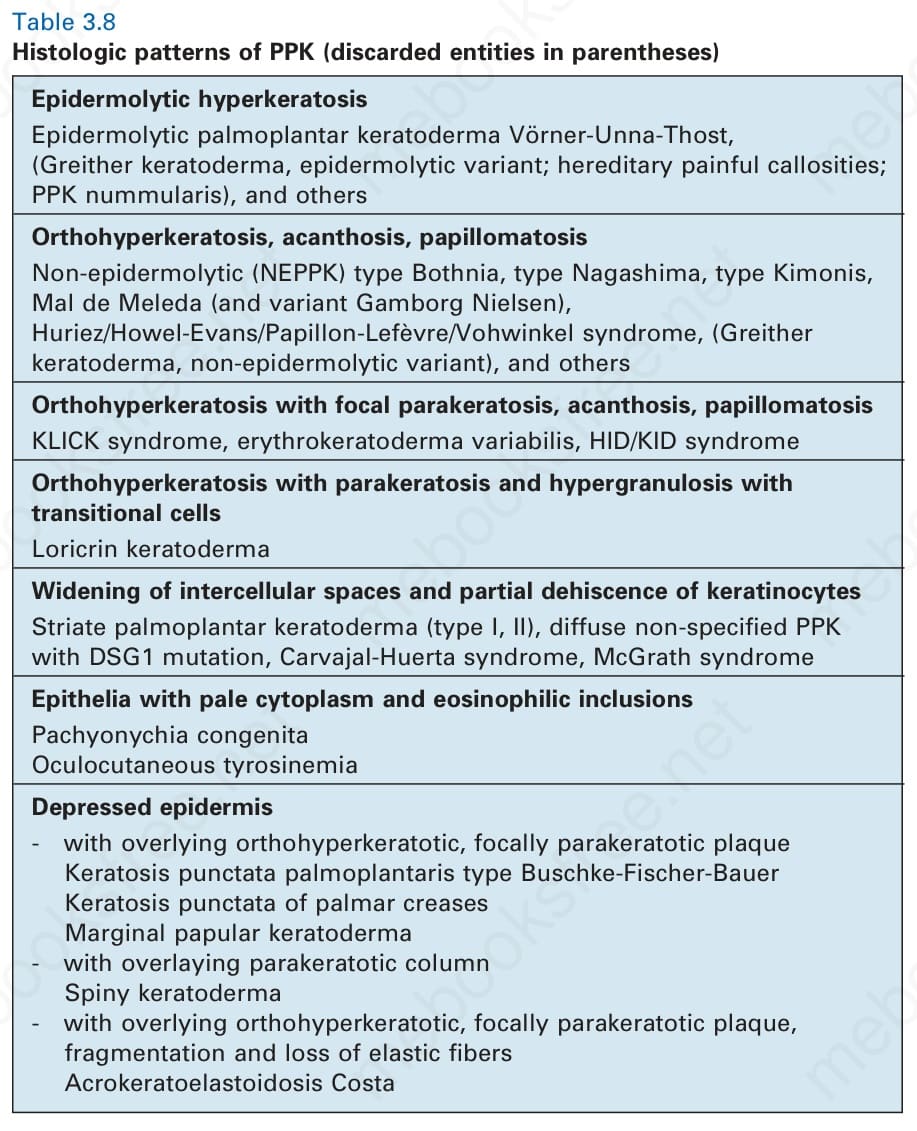
Table 3.8 Histologic patterns of PPK (discarded entities in parentheses)