Progressive symmetrical erythrokeratoderma
Progressive symmetrical erythrokeratoderma
Progressive symmetrical erythrokeratoderma (Gottron syndrome) is a non-migratory variant of erythrokeratoderma with large, fine scaly orange-red plaques with geographic borders that are symmetrically distributed on the shoulders, cheeks and buttocks (Fig. 3.74).1 Progressive symmetrical erythrokeratoderma may represent a manifestation of erythrokeratoderma variabilis as the same mutation in the gene GJB4 has been identified in affected individuals. Some of these patients express the variable form,2 while others develop the progressive symmetrical form of the disease.3 In addition the coexpression of both variants of erythrokeratoderma clinically, histologically, and ultrastructurally has been reported in siblings.4
Keratitis-ichthyosis-deafness syndrome, hystrix-like ichthyosis with deafness, porokeratotic adnexal ostial nevus
Clinical features Keratitis-ichthyosis-deafness (KID) syndrome and hystrix-like ichthyosis- deafness (HID) syndrome are likely to represent a spectrum of phenotypic variability of the same connexin-26 mutation instead of separate entities.1 Interestingly, a mosaicism for this mutation has been described as porokeratotic adnexal ostial nevus (PAON), also known as porokeratotic eccrine ostial and dermal duct nevus or porokeratotic eccrine nevus (PEN).2
Newborns with KID syndrome may present generalized erythema or a diffuse scaling and a leathery skin. During infancy patients develop spiny hyperkeratosis around the flexures, elbows, and knees, and hystrix-like scaling on the limbs. Scattered follicular hyperkeratosis can be found on the trunk. Most characteristically, symmetrical, well-demarcated hyperkeratotic and warty plaques appear on scalp, ears, face, and occasionally the trunk and limbs (Fig. 3.75).3 Circumoral furrows may lead to a progeria-like appearance. Palmar and plantar involvement with accentuation of the skin markings has been likened to heavily grained leather.4
84 Disorders of keratinization
Squamous carcinoma of the tongue and skin as well as multiple hair follicle tumors including malignant pilar tumors may develop in young adults and can lead to metastases.5–8
Inflammation of the cornea with photophobia is usual and a vascularizing keratitis leads to severe visual impairment.4 The end result is destruction of the cornea by a pannus of vascular or fibrous tissue (keratoconus).3,9,10
Deafness is of the congenital neurosensory type, but is occasionally due to recurrent otitis media; conduction defects may also be present.3,4 It is often total and frequently present at birth.11–13
Ectodermal dysplasia is variably present and features include alopecia (either partial or complete, including eyebrows and eyelashes), small malformed teeth with increased caries, scrotal tongue, leukokeratosis, and a variety of dystrophic nail changes including fragility, hyperkeratosis, dysplasia, leukonychia, and aplasia.3,4
Additional features that may be detected include increased susceptibility to superficial and systemic chronic infections (viral, bacterial, and fungal),14,15 neuromuscular disease, retraction of the Achilles tendon, hypohidrosis, heat intolerance, and growth deficiency.3 Mental retardation is a rare feature.3
The HID syndrome shows congenital ichthyosis with hystrix-like keratosis, in particular on the trunk and on the extremities (Fig. 3.76). Keratitis of the eyes is less prominent in HID patients, but they also suffer from neurosensorial deafness, proneness to mycotic/bacterial skin infections, and skin cancer.1,16,17
conditions.18–23 Connexins are gap junction proteins that form inter- and intracellular channels for ion and molecule transfer, which is the basis for all cellular communication. Some of the GJB2 mutations do not simply inhibit channel formation, but rather result in high conductance hemichannels at the cell surface.24 The genotype/phenotype relationship between the various connexin 26 related conditions is not currently understood. It is important to note that the hearing deficiencies are often due to recessive mutations, whereas KID and HID syndrome are transmitted as autosomal dominant traits.18–13
PAON is a hyperkeratotic verrucous, hard epidermal nevus following the lines of Blaschko. Comedo-like papules and filiform keratosis have been described, as well as keratotic pits on the palms and soles. The disease is usually unilateral, but may also be bilateral with widespread distribution on the extremities, including palms and soles and, more rarely, the trunk. Focal anhidrosis, hair loss, onychodysplasia, and pruritus can occur. Noteworthy, a mother affected by PEN may give birth to a child affected by KID syndrome.2,29,30
Pathogenesis and histologic features Recurrent and novel GJB2 mutations encoding for connexin 26 have been detected not only in KID and HID syndrome, but also in many other
In biopsies of HID and KID syndrome the epidermis shows psoriasiform, pseudoepitheliomatous or verruciform hyperplasia (Figs 3.77 and 3.78).4 The granular cell layer appears partially absent or thin. A prominent and vacuolized stratum granulosum can be also observed and sometimes the nuclei of the keratinocytes are surrounded by empty spaces reminiscent of a bird’s eye (Figs 3.79 and 3.80A).25,26 The horny layer is orthohyperkeratotic or parakeratotic. Most characteristically, parakeratotic areas show tiny roundish nuclear remnants or shadow nuclei (Fig. 3.80B). The papillary
85 Palmoplantar keratoderma
A
B
lymphocytic infiltrate is found. The epidermis between the adnexae shows acanthosis, papillomatosis, and orthohyperkeratosis.29,30
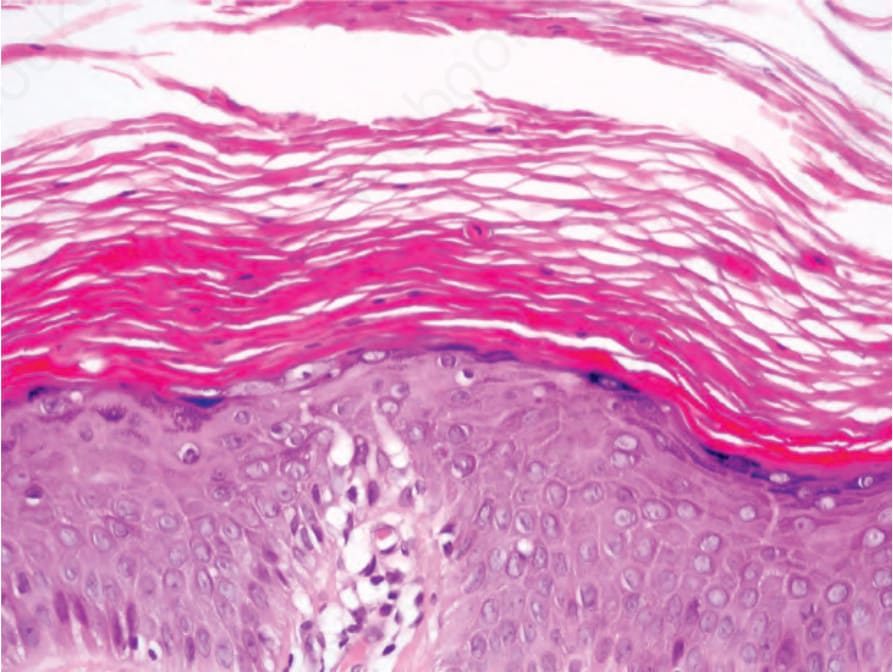
Fig. 3.73 Erythrokeratoderma variabilis: scattered dyskeratotic keratinocytes are sometimes seen.

Fig. 3.74 Progressive symmetric erythrokeratodermia: erythematous scaly plaques gradually appear on the extensor surfaces on the extremities and then persist.

Fig. 3.75 KID syndrome: there is marked scaling of the scalp with alopecia. Note the facial erythema and dark plaques on the cheeks. By courtesy of R.J.G. Rycroft, MD, St John’s Dermatology Centre, London, UK.

Fig. 3.76 HID syndrome: verrucous and hyperkeratotic, brownish-yellow sharply circumscribed plaques.
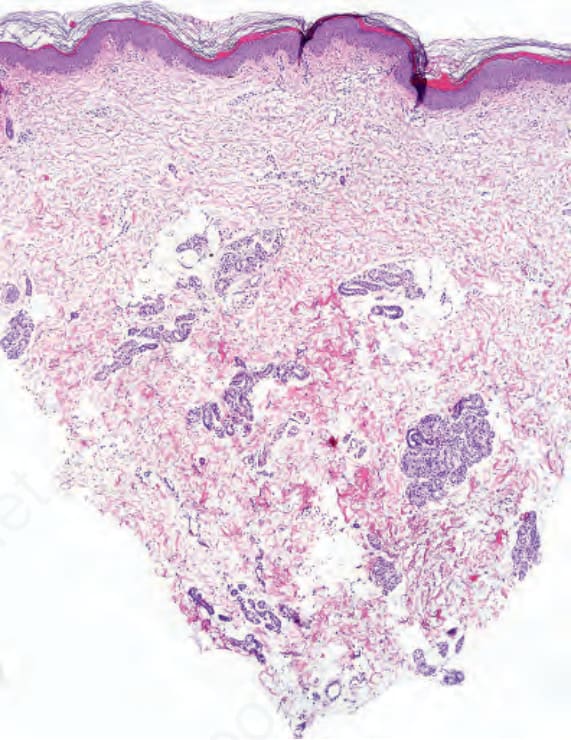
Fig. 3.77 KID syndrome: scanning magnification view showing mild hyperplasia of the epidermis. In this example the eccrine sweat glands are normal.
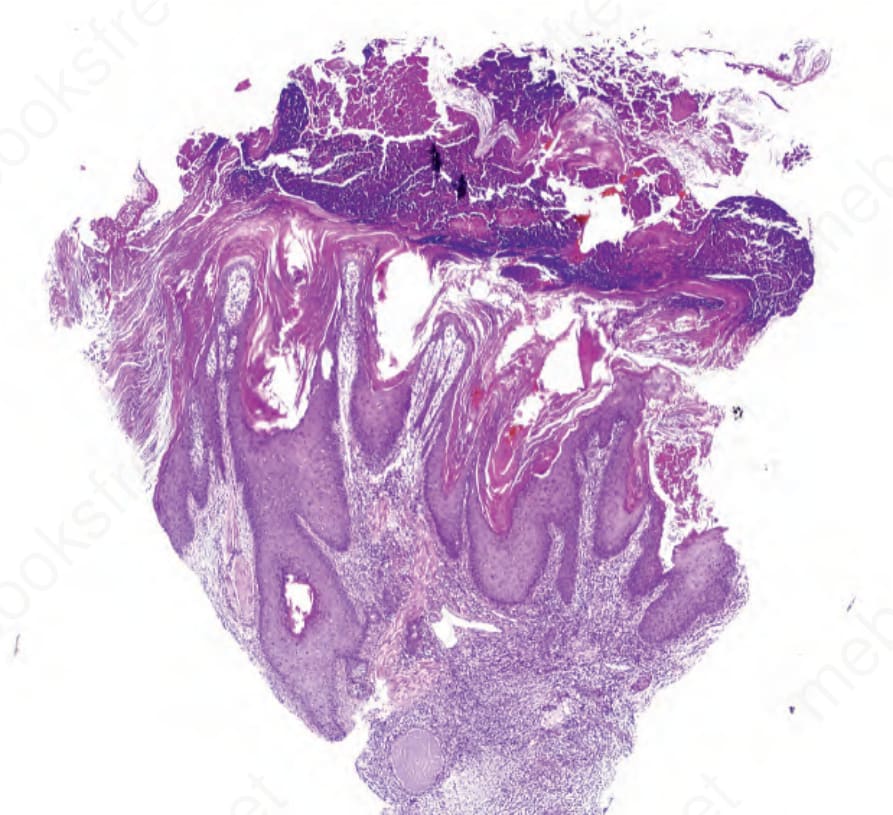
Fig. 3.78 HID syndrome: verrucous and pseudoepitheliomatous hyperplasia of the epidermis.
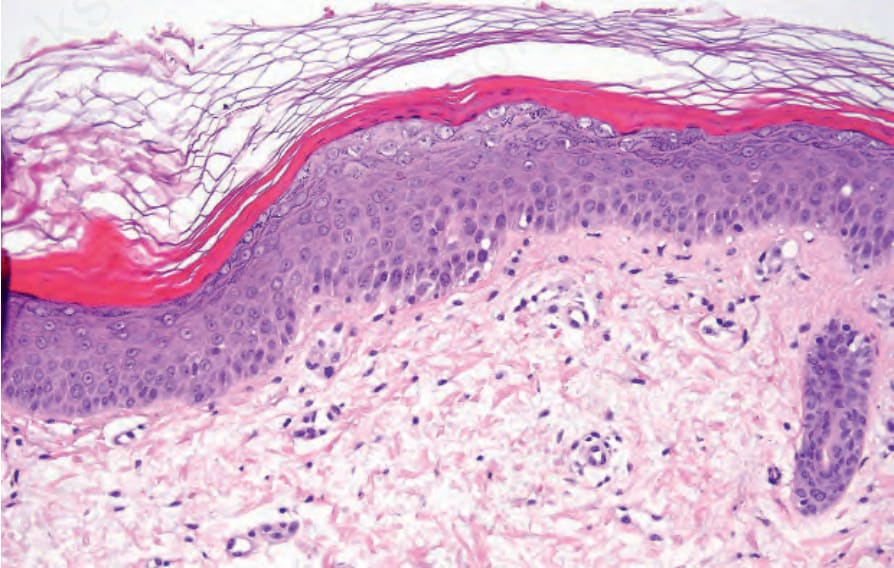
Fig. 3.79 KID syndrome: high-power view emphasizing the basket-weave keratin overlying a zone of compact keratin. There is focal parakeratosis and vacuolization of the granular layer.

Fig. 3.80 HID syndrome: the nuclei of the keratinocytes are surrounded by empty spaces reminiscent of a bird’s eye, (A) in the granular layer and (B) the horny layer.