Sjögren-Larsson syndrome
Sjögren-Larsson syndrome
Clinical features This autosomal recessive inherited disorder combines the features of ichthyosis, spastic bi- or quadriplegia and mental retardation.1–5 It is rare, with an incidence of 0.4 per 100 000 of the population albeit it has a higher prevalence of 1 : 10 000 in Northern Sweden. 2,4
The ichthyosis, which develops in the first year of life with diffuse scaling, affects the entire body with the exception of the central face and is typically intensely pruritic (Fig. 3.51).3,5 Later, the skin has a brownish-yellow color and shows a cobblestone-like lichenification.4 Hyperkeratosis around the
Visual acuity is often impaired and photophobia is a frequent complaint. Macular degeneration associated with crystal deposition is characteristic (Fig. 3.52).6
Pathogenesis and histologic features Sjögren-Larsson syndrome results from deficiency of microsomal fatty aldehyde dehydrogenase (FALDH).7 The gene has been mapped to 17p11.2 and multiple mutations, including missense mutations, deletions, and insertions, have been identified.8–10 In the pathophysiology of the ichthyosis a disturbed hepoxilin pathway is involved, while an abnormal lipid composition of myelin accounts for the neurological defects.6 The abnormal level of free fatty alcohols in cultured fibroblasts, direct testing of FALDH activity, or
74 Disorders of keratinization
A
B
Pathogenesis and histologic features Refsum syndrome is generally caused by a mutation in the PHYH gene encoding peroxisomal phytanoyl-CoA hydroxylase.3,4 Mutations in the peroxisomal receptor gene PEX7 account for adult forms.5–7 Peroxisomes are involved in the metabolism of bile acid and cholesterol biosynthesis. Elevated levels of phytanic acid in plasma and tissue are diagnostic. Therapy includes a low-phytol diet and apharesis.8,9
the presence of LTB4 metabolites in urine can provide biochemical screening and/or confirmation of the clinical diagnosis, prior to molecular mutation analysis of the FALDH gene.5
Histologically, there is papillomatosis, acanthosis, and basket-weave hyperkeratosis with scattered mild parakeratosis and occasional follicular hyperkeratosis (Fig. 3.53). Epidermal hyperproliferation has been demonstrated.11,12 The granular cell layer may be slightly thickened. A moderate lymphocytic infiltrate is sometimes present around the superficial dermal vasculature.
Routine histology of a skin biopsy does not differ from ichthyosis vulgaris. When a biopsy is fixed in alcohol and a Sudan stain performed, lipid droplets are found in the keratinocytes, in particular in biopsies from melanocytic nevi. The same inclusions can be shown by ultrastructural examination.10,11

Fig. 3.51 Sjögren-Larsson syndrome: brownish-yellow color and a cobblestone-like pattern of lichenification is typical. By courtesy of M. Willemsen, MD, University Medical Center, Nijmegen, Belgium.
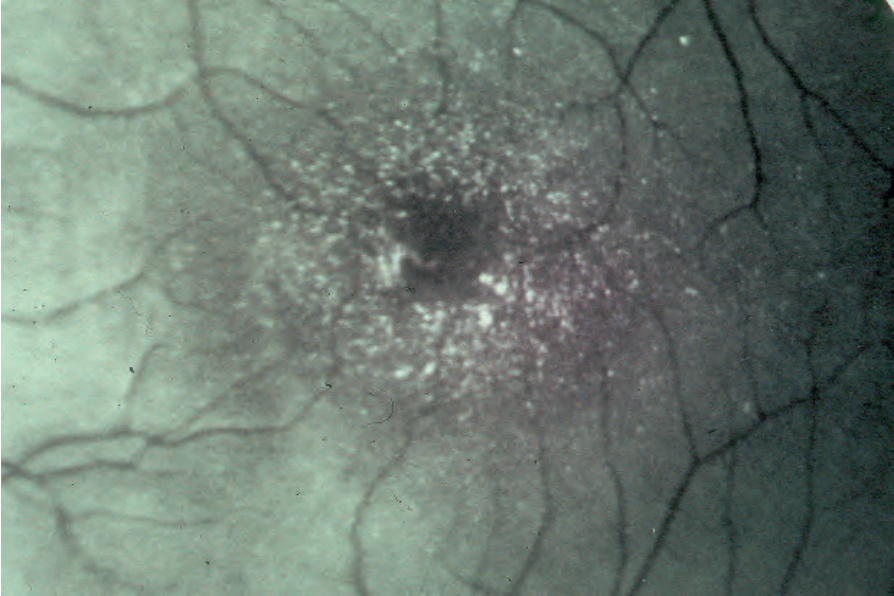
Fig. 3.52 Sjögren-Larsson syndrome: characteristic macular crystals. By courtesy of M. Willemsen, MD, University Medical Center, Nijmegen, Belgium.
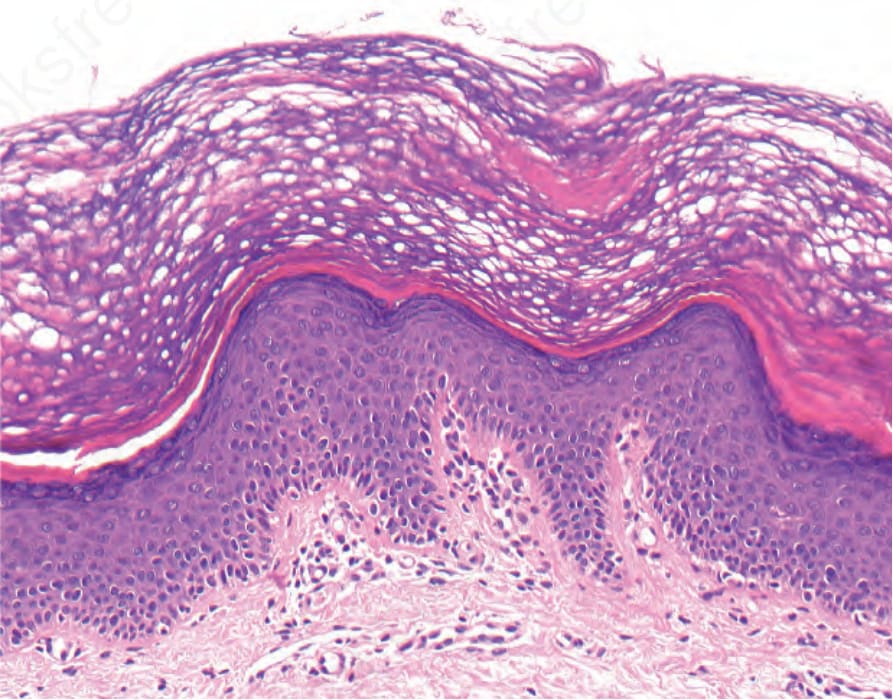
Fig. 3.53 Sjögren-Larsson syndrome: there is hyperkeratosis, with focal parakeratosis, hypergranulosis, and mild papillomatosis. A mild superficial perivascular lymphocytic infiltrate is present.
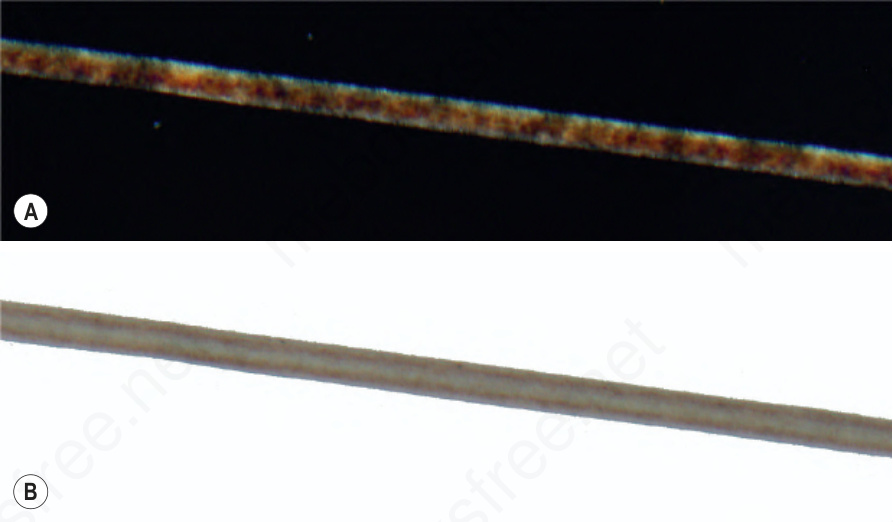
Fig. 3.54 Trichothiodystrophy: (A) polarizing microscopy of a hair shows an alternating light and dark banding (‘tiger-tail pattern’). (B) The same hair without polarizing.