Comèl-Netherton syndrome
Comèl-Netherton syndrome
Clinical features Comèl-Netherton syndrome (Netherton syndrome, ichthyosis linearis circumflexa) is a rare autosomal recessively inherited genodermatosis. It is characterized by the triad of CIE, hair shaft anomalies, and a severe atopic diathesis with high IgE blood levels and eosinophilia.1 It is believed to affect approximately 1 : 200 000 of the population.2 Generally, the CIE gradually evolves into a milder ichthyosis linearis circumflexa which is characterized by an erythematous, scaly rash predominantly affecting the trunk and limbs.3 It is composed of polycyclic, migratory, annular and serpiginous lesions with characteristic two parallel lines of scale at the periphery, the so-called
For histologic diagnosis, the biopsy should be taken from the scaly margin. A sample from this area will reveal the diagnostic psoriasiform features while biopsies from the center of the lesion show misleading features of atopic dermatitis.
70 Disorders of keratinization
A
A
B
Netherton syndrome shows a psoriasiform dermatitis with parakeratosis and intracorneal neutrophils (sometimes with formation of Munro microabscesses) often indistinguishable from psoriasis vulgaris (Fig. 3.45).6 New findings described in a series of patients, include compact parakeratosis with large nuclei, subcorneal or intracorneal splitting, presence of clear cells in the upper epidermis or stratum corneum, dyskeratosis, elongated rete ridges without suprapapillary thinning and a superficial dermal inflammatory cell infiltrate rich in neutrophils and/or eosinophils.18 Small, dark, round or oval granules can be identified within the stratum granulosum.19 They are diastase-resistant, and periodic acid-Schiff (PAS) and Sudan black
B
positive and are thought to represent an influx of serum exudates resulting from the accompanying dermal inflammation. Similar ‘inclusions’ have been described in psoriasis and atopic eczema and as such they are not specific.19
Electron microscopy reveals reduced numbers of LBs in keratinocytes and the presence of lysosomal inclusion bodies with intercellular amorphous deposits in the horny layer.20,21
Immunohistochemistry can demonstrate the absence of LEKTI antigen and is highly specific for the Netherton syndrome both in neonatal
71 Ichthyosis
A
erythroderma and scaly rashes of adults.22,23,24 A definite diagnosis can be made by negative staining for LEKTI in the inner root sheath of hair follicles since Netherton syndrome and other diseases may lack the stratum granulosum where LEKTI is normally expressed.18 However, residual LEKTI expression in the outer epidermis is still demonstrable immunohistochemically in mild forms of Netherton syndrome.25
Differential diagnosis Distinction from psoriasis vulgaris may be histologically extremely difficult (if not impossible) in the absence of clinical information. Other genodermatoses, dermatophytosis, and inflammatory skin diseases with a psoriasiform-like pattern must be differentiated (see Table 3.3). Netherton syndrome shares the distinct histologic feature of corneal splitting with other exfoliative disorders of cornification, such as peeling skin syndrome (PSS) and severe dermatitis, multiple allergies, metabolic wasting syndrome (SAM). Atopic dermatitis is another important differential diagnosis.
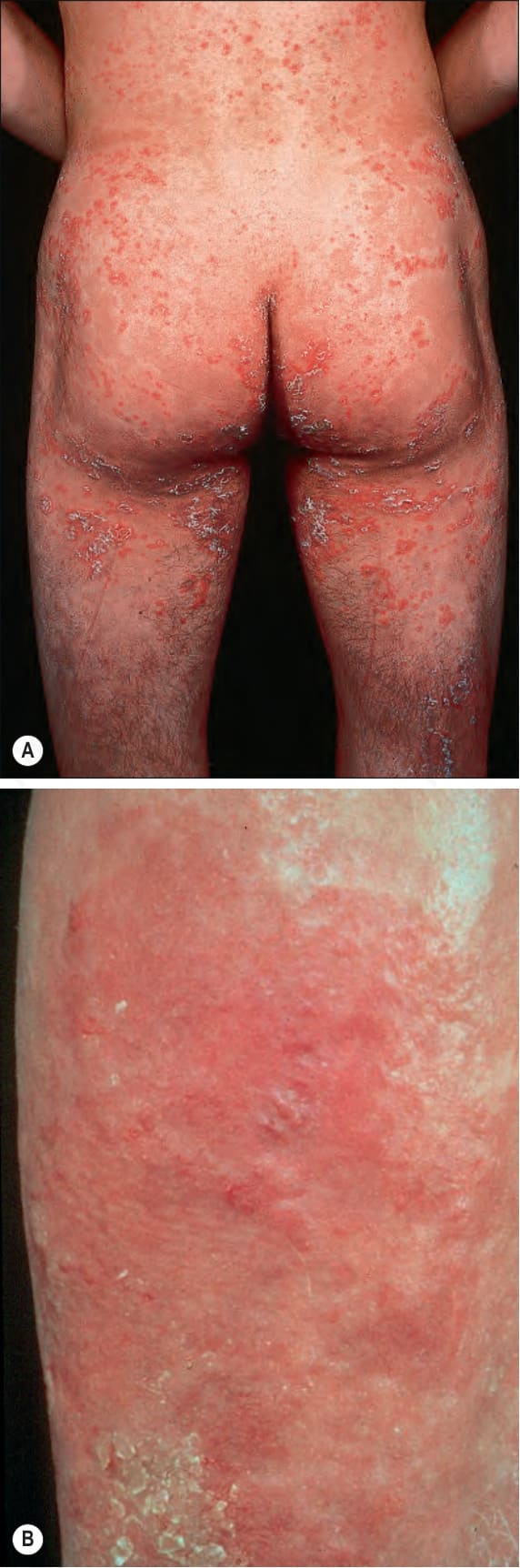
Fig. 3.42 Comèl-Netherton syndrome: (A) hyperkeratotic lesions may sometimes be prominent; (B) note the focal loss of the polycyclic pattern.

Fig. 3.43 Comèl-Netherton syndrome: (A) there is profound erythema with scaling; (B) the hair is dull and appears short and thin. The eyebrows are deficient. (A) By courtesy of M. Judge, MD, Institute of Dermatology, London, UK. (B) By courtesy of A. Griffiths, MD, Institute of Dermatology, London, UK.

Fig. 3.44 Comèl-Netherton syndrome: bamboo hair (trichorrhexis invaginata). By courtesy of M. Judge, MD, Institute of Dermatology, London, UK.
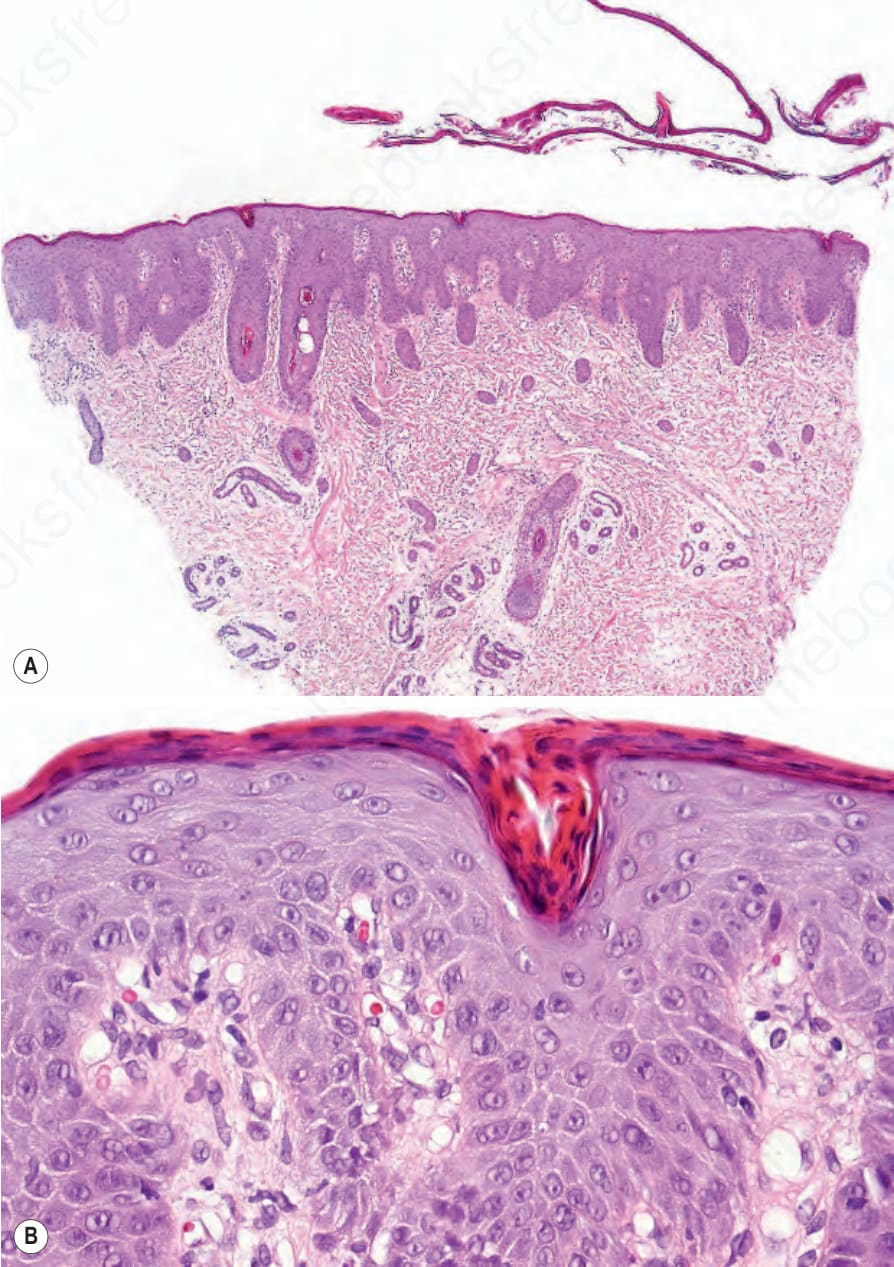
Fig. 3.45 Comèl-Netherton syndrome: (A) scanning view showing a detached thickened stratum corneum and psoriasiform hyperplasia; (B) note the marked parakeratosis and dilated vessels mimicking psoriasis vulgaris.
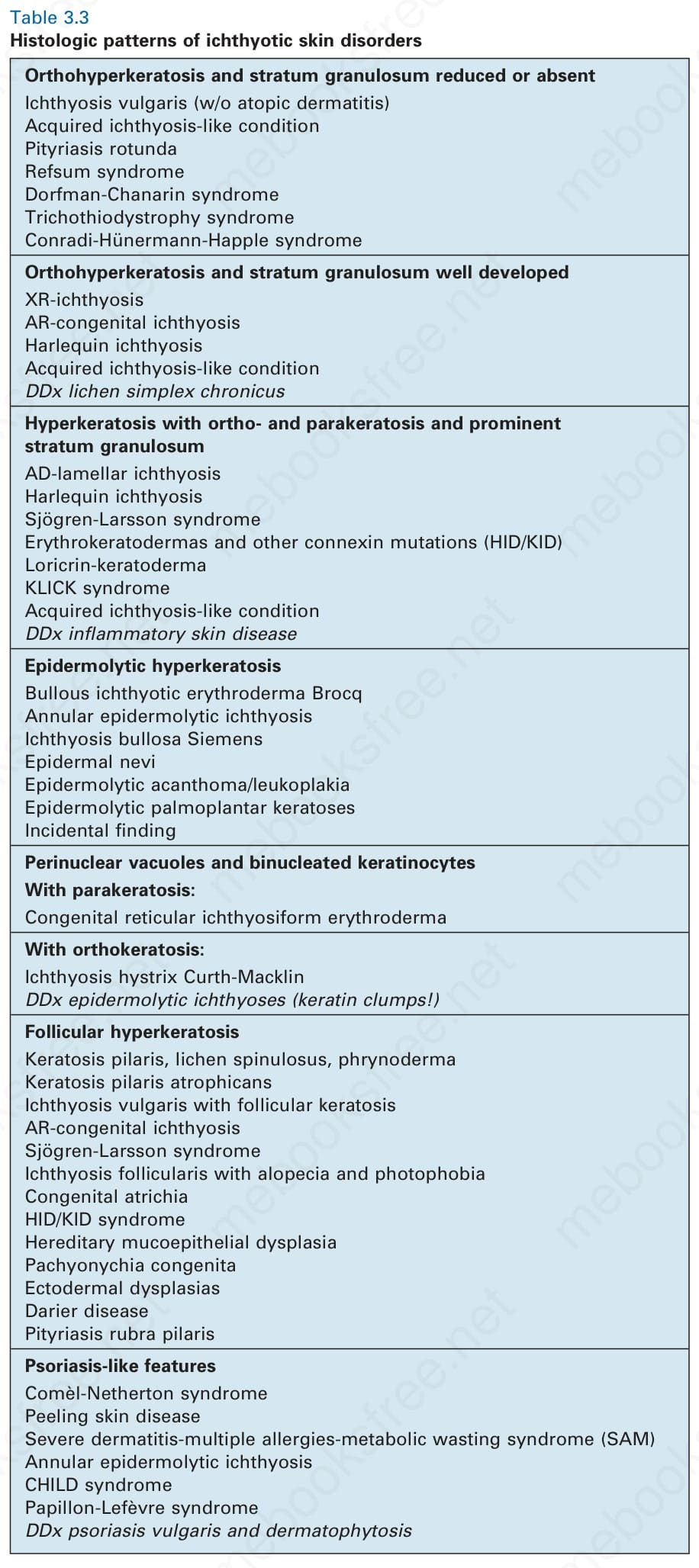
Table 3.3 Histologic patterns of ichthyotic skin disorders