Epidermolytic ichthyosis
Epidermolytic ichthyosis
Epidermolytic ichthyosis (EI) is a rare autosomal dominant disease (incidence of 1 : 300 000 births), but it often arises by a spontaneous mutation.1–3 At birth infants may show marked erythroderma and develop widespread blistering (Fig. 3.23). Therefore, a major differential diagnosis is epidermolysis bullosa. As the patient becomes older, the erythema and blistering become less apparent and, later, the disease is complicated by the development of verrucous hyperkeratosis, especially in the flexures (Figs 3.24–3.28). The descriptive word ‘hystrix’ (porcupine) for this cobblestone-like appearance of the skin has been abandoned. The nape, axilla, groin, and flexural folds are sites of predilection. Severe involvement of the scalp may simulate tinea capitis. Occasional blisters still arise at sites of mechanical stress, often in summer or when the patients have fever and skin infections. Many patients suffer from an offensive body odor. Neonates with EI have an increased risk of sepsis, fluid loss, and electrolyte imbalance.1–2 Patients with KRT1 mutation often develop severe, sometimes painful palmoplantar keratoderma. Nail dystrophy may also occur. Therapeutic administration of systemic retinoids may aggravate the complications, especially in patients with KRT1 mutation.3
Epidermolytic hyperkeratosis as seen in some types of epidermal nevus is the result of somatic mutations in KRT1 or KRT10.8 A specific histologic
Pathogenesis and histologic features First, it was shown that EI shows linkage to the keratin gene cluster either on chromosome 12q11–13 (type II keratin) or chromosome 17q21-q22 (type I keratin)4–6 and that transgenic mice expressed a mutant KRT10 gene.7 This was followed by detection by direct DNA sequencing of a point mutation in KRT1 or KRT10 in a number of affected families.8–14 Most mutations are missense mutations and clustered at the ends of the central helical rod domains. KRT1 mutations typically affect palmoplantar skin. This region is
64 Disorders of keratinization
most often spared in EI with KRT10 mutation, which can be explained by its physiological substitution of keratin 9 on palmoplantar skin.1
EI shows the typical features of epidermolytic hyperkeratosis.15–17 Suprabasal keratinocytes appear vacuolated and typically contain distinct eosinophilic intracytoplasmic inclusions. The cell borders are ill defined and
intraepidermal blister formation may be present. There is massive orthohyperkeratosis, papillomatosis, and acanthosis. The granular cell layer is prominent and contains coarse and irregular keratoyhaline granules (Fig. 3.29).
By immunohistochemistry, epidermolytic hyperkeratosis shows a normal distribution pattern of keratins 5/14 and 1/10, but in addition, there is overexpression of keratin 14 in the suprabasal epithelium accompanied by quite marked labeling of the upper epithelial layers by keratin 16, as would be expected in a hyperproliferative state.18
Ultrastructural studies have shown that the intracytoplasmic inclusions seen on light microscopy are composed of abnormally aggregated keratin filaments. Since large areas of the cytoplasm lack a regular keratin skeleton,
65 Ichthyosis
A
the suprabasal keratinocytes appear vacuolated and contain irregular keratoyhaline granules. Impairment of desmosome-keratin complexes accounts for the fragility of the epidermis (Fig. 3.30). Immunoelectron microscopy has identified that the keratin clumps are composed of keratins 1 and 10.18 These ultrastructural changes may form the basis of prenatal diagnosis including amniotic fluid squame analysis.16–17
B

Fig. 3.23 Congenital bullous ichthyosiform erythroderma: close-up view of an infant showing intense erythema and blistering. By courtesy of M. Liang, MD, The Children’s Hospital, Boston, USA.

Fig. 3.24 Epidermolytic ichthyosis: hyperkeratosis and scales follow re-epithelialization of widespread blistering.

Fig. 3.25 Epidermolytic ichthyosis: adult showing very generalized scaling, particularly severe on the legs. By courtesy of the Institute of Dermatology, London, UK.
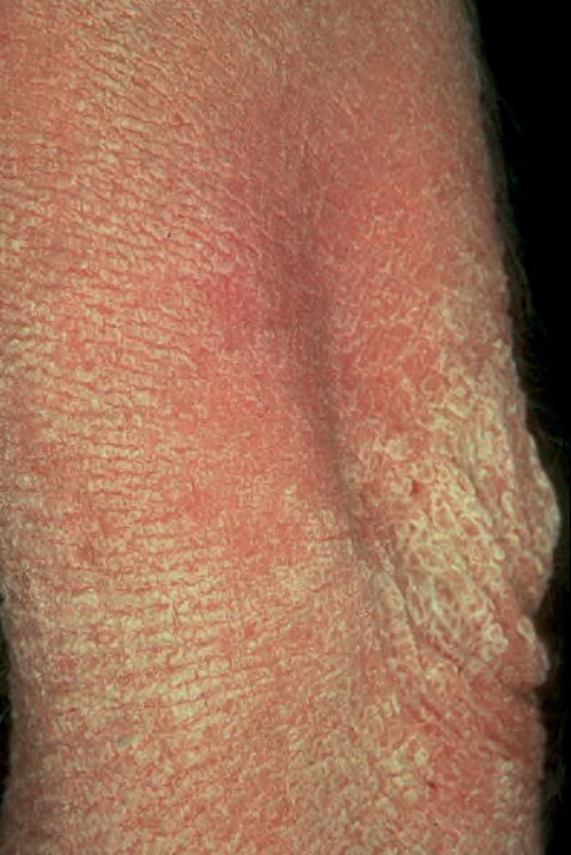
Fig. 3.26 Epidermolytic ichthyosis: same patient as Figure 3.25, showing elbow involvement with verrucous hyperkeratosis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 3.27 Epidermolytic ichthyosis: the hands are particularly affected. By courtesy of the Institute of Dermatology, London, UK.

Fig. 3.28 Epidermolytic ichthyosis: blistering may sometimes be seen in adulthood. By courtesy of the Institute of Dermatology, London, UK.
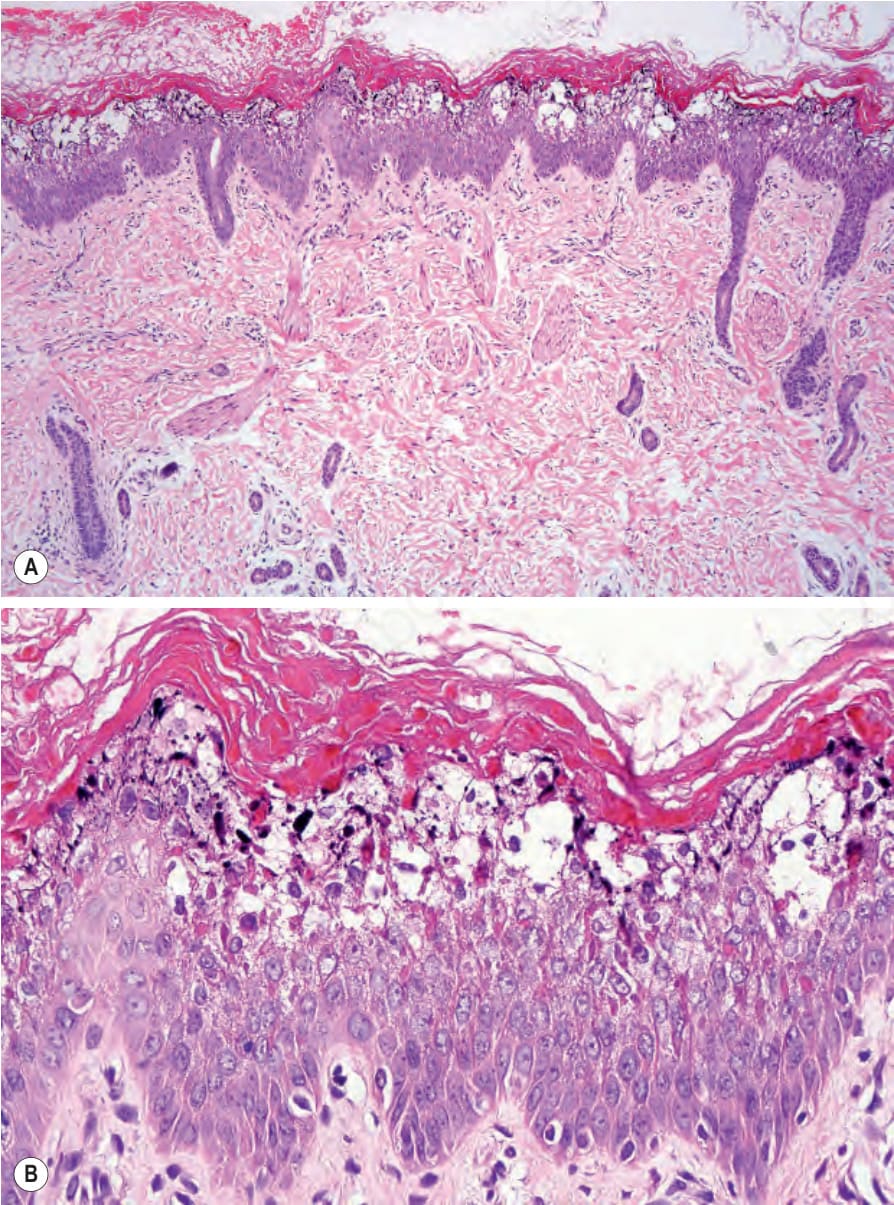
Fig. 3.29 Epidermolytic ichthyosis: (A) there is massive hyperkeratosis and acanthosis. The epidermis shows conspicuous superficial vacuolation, which has resulted, in vesiculation; (B) there is intracellular vacuolation, and irregular eosinophilic granules (representing dense abnormal aggregates of keratin filaments) are present in the superficial layers of the epidermis.
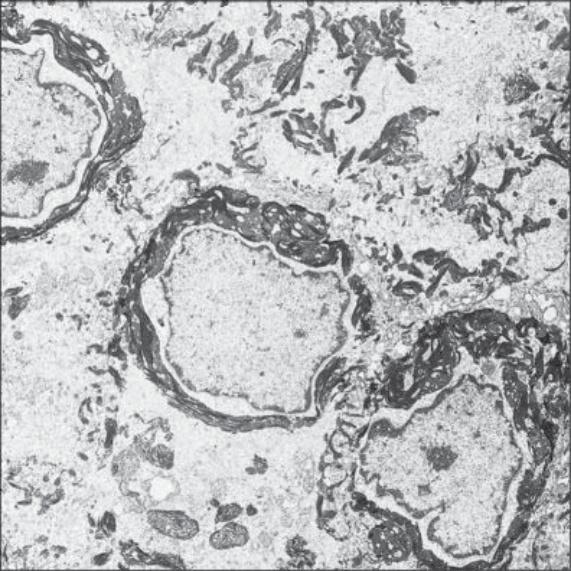
Fig. 3.30 Epidermolytic ichthyosis: striking perinuclear keratin clumping is evident. By courtesy of R.A.J. Eady, MD, Institute of Dermatology, London, UK.