Allelic imbalance
Allelic imbalance
Gains or losses of specific regions of DNA, often containing particular genes of interest, can provide diagnostic insight.
has led to decreased emphasis on transmission electron microscopy as a diagnostic tool in EB.6 Ultrastructural analysis, however, can be useful in confirming the plane of cleavage and in establishing the diagnosis of certain dominant forms of EB. Skin from the neonate illustrated in Fig. 2.17B, for example, shows normal intensity basement membrane zone reactivity for all diagnostic probes but transmission electron microscopy (Fig. 2.21) identifies discrete clumps of tonofilament and basal keratinocyte cytolysis, characteristic of the generalized severe variant of autosomal dominant EB simplex. For recessive forms of EB, however, skin immunolabeling has become the most important diagnostic approach.7 Reduced or absent staining for a particular protein provides a rapid diagnosis as well as a means of identifying the encoding gene (or genes) in which the underlying pathogenic mutations are present. Thus the skin biopsy findings, both histologic and immunohistochemical, provide a direct guide to molecular screening tests, most of which are PCR-based or next-generation sequencing (NGS)–based, as discussed below. For dominant forms of EB, however, skin immunohistochemistry of patient skin may be indistinguishable from normal control skin and therefore Sanger sequencing of DNA is often preferred to skin biopsy analysis as the initial diagnostic investigation.6 Indeed, DNA sequencing is the optimal method for diagnosing the most common form of EB, localized EB simplex (blisters mainly on the hands and feet, which accounts for > 70% of all cases of EB). Furthermore, the diagnosis of EB is increasingly embracing NGS technologies, including whole exome sequencing and selected gene panels, as primary diagnostic tools.7 This molecular information can then be used for genetic counseling, carrier screening, and DNA-based prenatal testing, if indicated. Nevertheless, a clear advantage of skin biopsy diagnostics for EB is time to diagnosis: skin immunohistochemistry can be completed within 2 days and thus skin biopsy is likely to remain a key part of EB diagnostics, particularly in the diagnosis of neonates with EB, for the foreseeable future.
An allele is a variant of a particular genetic locus or region of DNA such as a gene. Detection of allelic imbalance or loss of heterozygosity (LOH) is a method that can detect the presence of deletions or gains of specific alleles in paraffin-embedded material.5 This usually corresponds to regions of a particular gene(s) of interest. For this approach, PCR is used to amplify small genomic fragments that carry common polymorphisms and thus have a high likelihood of being present in two different variants (alleles) in an individual. Ideally, these variants are of different size so that they can easily be detected on an electrophoretic gel; DNA sequencing can be used if this is not possible. Only if two different alleles in the normal tissue of a patient are present is this technique informative. Imbalance (loss of one allele) is implied if one detects only one of the alleles in the tumor tissue, or more commonly a vast excess of one allele since normal tissue is present with the tumor cells. More detailed analysis can distinguish those that are true losses. Sites of recurrent losses are typically areas that harbor tumor suppressor genes. This method can detect losses that would not be demonstrated in a traditional chromosomal karyotype analysis and can be readily adapted to formalin-fixed, paraffin-embedded (FFPE) tissue. The limitations of LOH analysis include that it is sensitive to contamination by normal (stromal) cells that with increasing amounts can make it difficult to decide whether an allele is lost. Another drawback is its inability to determine whether the imbalance is caused by the loss of one marker or by a copy number increase of the other marker.
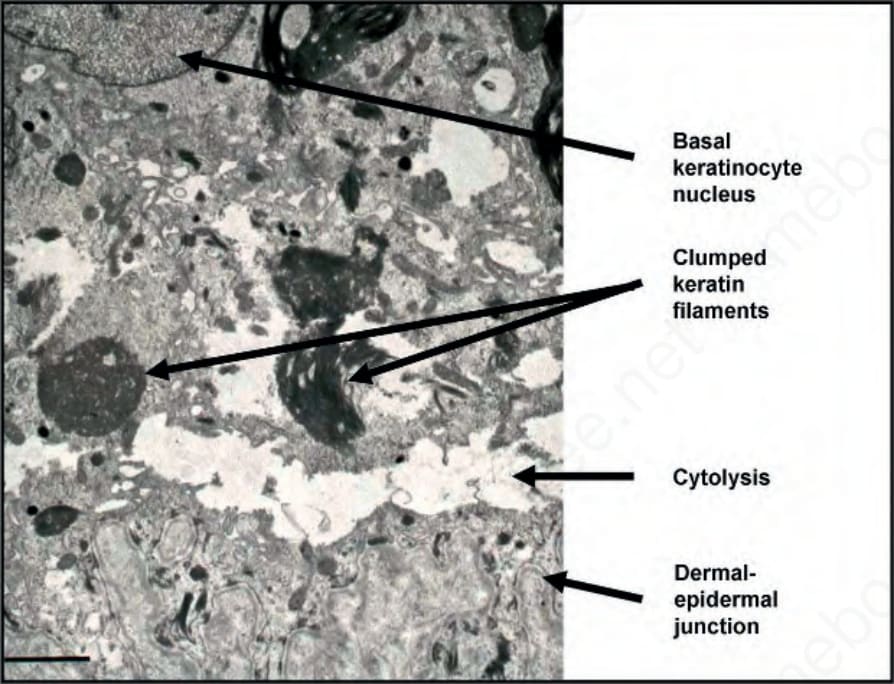
Fig. 2.21 Transmission electron microscopy of skin in Dowling-Meara EB simplex (case illustrated in Fig. 2.17B): within the basal keratinocyte cytoplasm the keratin filaments are condensed and form clumps and there is cytolysis that occurs just above the dermal–epidermal junction. (Bar = 1 µm.)