Specialized techniques in
Specialized techniques in
for references and additional material
2
dermatopathology
Pratistadevi K. Ramdial, Boris C. Bastian, Jeffrey P. North, John Goodlad,
John A. McGrath and Alexander J. Lazar
Specimen fixation, grossing/put-
Frozen section examination of skin
through, processing, embedding and sectioning 35 Routine and ‘special’ stains 35 Immunohistochemical techniques 37 Immunohistochemical techniques and
Polymerase chain reaction (PCR) 48 Next-Generation Sequencing (NGS) 49 Diagnosis of lymphomas 50 PCR analysis of cutaneous lymphoid infiltrates 50 T-cell receptor gene rearrangement in cutaneous
specimens 41 Diagnostic cytopathological techniques in
dermatopathology 42 Diagnosis of inherited skin diseases 42 Molecular techniques 44 Chromosomal karyotyping 44 Allelic imbalance 44 Fluorescence in situ hybridization (FISH) 44 Comparative genomic hybridization (CGH) 47
trouble shooting 39 Immunofluorescence 40 Electron microscopy 41
lymphoproliferations 51 IG gene rearrangement in cutaneous
lymphoproliferations 51
Specimen fixation, grossing/put-through, processing, embedding and sectioning
The aim of fixation is to maintain clear and consistent lesional features and to preserve tissue in an optimal state suitable for a range of staining and ancillary histopathological techniques.1,2 Most fixation methods employed during tissue processing depend on chemical fixation of tissue in liquid reagents.3 Tissue fixation may also be accomplished by physical (heat, microwave, freeze-drying, and freeze substitution) and/or chemical (coagulant and cross-linking) methods.4 The most commonly used fixative is 10% neutral-buffered formalin solution with a pH between 7.2–7.4. It prevents the formation of formalin pigment in tissue sections. The quality of fixation is affected by:
• the size of the specimen,
• duration and temperature of fixation,
• pH,
• concentration,
• osmolality,
• ionic composition of fixatives and additives contained in the fixative.5
Tissue processing refers to a series of steps that effect the removal of extractable water from biopsies to ensure sections of optimal diagnostic quality.9 These include fixation, dehydration, clearing, infiltration, and embedding in a support matrix. Use of manual and automated tissue processing achieves this goal, including:
• carousel-type processors,
• self-contained vacuum infiltration tissue processors (Fig. 2.2),
• microwave tissue processing. In most laboratories, overnight processing runs are the norm.9 However, microwave-assisted tissue processing facilitates shorter processing times of 1–2 hours. Dehydrating reagents promote the removal of unbound water and aqueous fixatives from the tissue. Clearing reagents serve as an intermediary between the dehydrating and infiltrating solutions, being miscible with both. Paraffin is the most popular infiltration and embedding medium, being suitable for the majority of routine and special stains. The important principle to be adhered to during embedding of skin biopsies is that the orientation of the skin sample should offer the least resistance to the blade during microtomy (Fig. 2.3). Skin biopsies are usually cut in a plane at right angles to the epidermis so as to minimize its compression and distortion.
Formalin fixation occurs at an approximate rate of 1 mm per hour.4,6,7 The volume of the fixative should ideally be at least 10 times the volume of the specimen.7 Large specimens, such as tumors, may require sectioning into 5-mm thick slices, covering with fixative-soaked gauze or cloth and fixation overnight.5,7
Suboptimally processed tissue may result in incomplete tissue sections and expansion or disintegration of sections in the water bath. Incorrectly embedded tissue may result in poorly orientated incomplete sections. Faulty microtome mechanisms; loose, dull, or damaged blades; and inaccurate clearance angles may be the causes for:
• thick and thin sections,
• folds (Fig. 2.4),
• holes (Fig. 2.5),
• scores (Fig. 2.6),
• chatter.10
Diagnostic dermatological biopsies may be:
• small incisional (shave, core, punch),
• excisional specimens.8
Prior to put-through, excisional specimens that require an appraisal of margins should be inked. If localization sutures have been inserted by surgeons then four-quadrant, four-color painting or two-color painted halves (Fig. 2.1) is usually appropriate. Shave biopsies are used to sample or remove lesions and, if of appropriate size, may be divided into sections, bisected or trisected and embedded on edge. Edge embedding is critical in a shave excision of a lesion such as a small melanoma so that both the width and depth of invasion can be quantified.8,9 The main purpose of core or punch biopsies, which generally measure 2–8 mm in diameter, is for diagnostic sampling of larger lesions. Biopsies larger than 4 mm in size should be bisected and the specimens embedded with the cut surfaces down. The bisectioning and embedding cut surface down ensures that the lesion is not missed. Biopsies less than 4 mm are put through in toto.9,10
The presence of calcified areas and suture in skin tissue and nicks in the blade may result in chatter or splitting of sections at right angles to the knife edge.
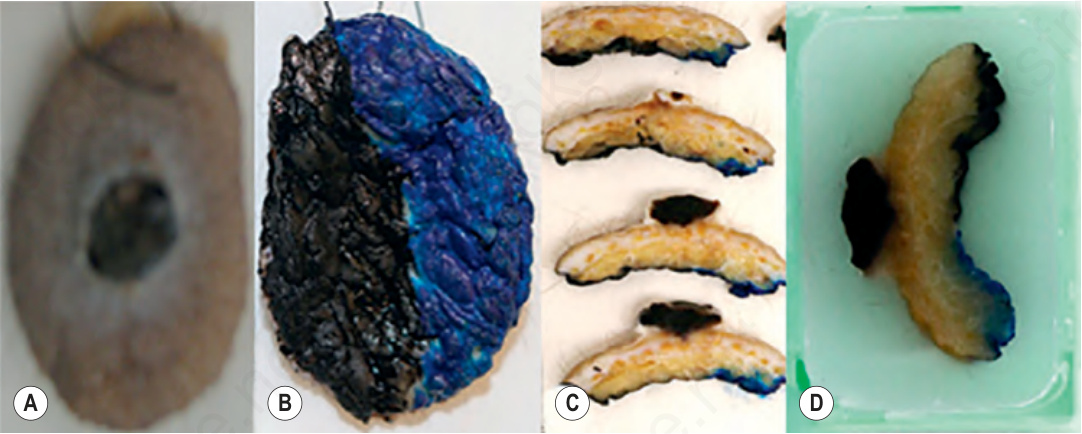
Fig. 2.1 Gross representation of pyogenic granuloma (A), with two-color painting of the inferior surface (B). 2-mm– thick gross sections demonstrating the black and blue painting at put-through (C) and in paraffin blocks (D). By courtesy of K. Nargan and K. Lumamba, Africa Health Research Institute, Durban, South Africa.

Fig. 2.2 A self-contained vacuum infiltration tissue processor of fluid-transfer type.
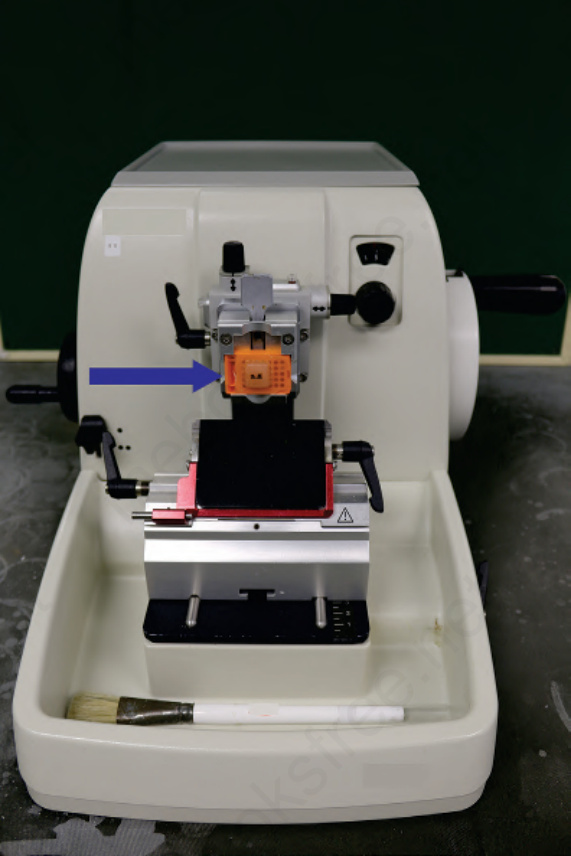
Fig. 2.3 Paraffin block containing skin tissue (arrow) on microtome.
Fig. 2.4 Technical artifact: folds in tissue sections because of poor bath floating technique.
Fig. 2.5 Technical artifact: holes in tissue sections caused by excessively thin sectioning.
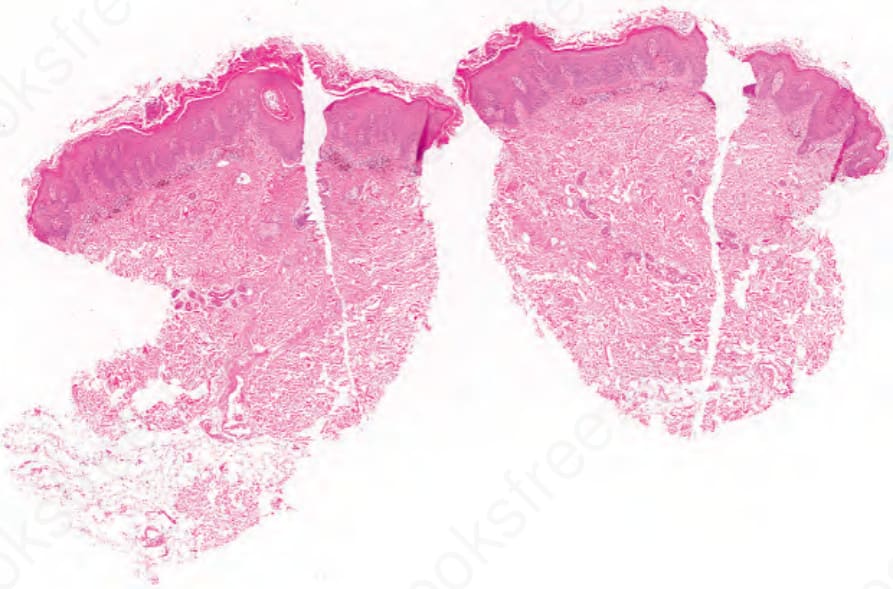
Fig. 2.6 Technical artifact: vertical scores in tissue sections caused by a damaged microtome blade. By courtesy of K. Nargan, Africa Health Research Institute, Durban, South Africa.