Porokeratosis
汗孔角化症 (porokeratosis)
臨床特徵 (Clinical Features)
- 典型的環狀病灶 (annular lesions) 具有隆起的角化過度邊緣 (raised hyperkeratotic margin)(見第 3 章),分布上典型為全身廣泛性 (generalized),但肛門生殖器皮膚 (anogenital skin) 也可能受累。
- 少見情況下,生殖器皮膚單獨受累 (genital porokeratosis);更罕見者,可見限於肛周與臀褶 (perianal and gluteal folds) 的搔癢性、偶呈疣狀 (verrucous) 之受累 (porokeratosis ptychotropica)。
- 鑑別診斷包含 LP 與 amyloid(後者曾在 porokeratosis ptychotropica 中被報導)。曾有與骨髓移植 (bone marrow transplantation) 相關的描述。
- 發病率有兩個高峰;在女性,這些高峰出現於青春期前 (prepubertal years) 及停經後 (post-menopause);在男性則出現於青春期前及青年至中年成年男性。當疾病於兒童期發生時,傾向於持續存在,消退並不常見。
- 在女孩,此病可在極早年齡即以出血性肛周病灶 (hemorrhagic perianal lesions) 表現 (Figs 12.48 and 12.49)。便祕 (Constipation) 可作為肛管疼痛性裂隙 (painful fissuring of the anal canal) 的併發症而發生。若有明顯的肛門生殖器受累,此病可能被誤認為性虐待 (sexual abuse)。
- 肛周疾病不發生於男性,但在男孩,genital LS 是包莖 (phimosis) 最常見的原因。在患有 genital LS 的女性中,有 11% 出現生殖器外病灶 (Extragenital lesions)。
- 此種受累依頻率遞減順序出現於上軀幹 (upper trunk)、腹股溝 (groins)、上肢 (upper extremities)、頸部 (neck)、下軀幹 (lower trunk) 與下肢 (lower extremities),通常位於摩擦 (friction) 部位 (Figs 12.50 and 12.51)。
- 頭皮與顏面受累罕見,且可與禿髮 (alopecia) 相關。曾記錄一例罕見的足底 (plantar) 受累。
- 在無生殖器病灶的情況下出現生殖器外病灶極為罕見。Koebner 現象 (Koebner phenomenon) 常見,且 LS 曾被描述與瘢痕 (scars)、放射治療 (radiotherapy) 部位、胰島素注射 (insulin injection) 部位以及刺青 (tattoo) 相關。病灶也可在皮膚或肌皮移植片 (skin or myocutaneous grafts) 中發生或復發。
- 曾有口腔受累 (Oral involvement) 的描述,包括以唇部病灶 (lip lesions) 為孤立現象,或與生殖器病灶相關。後者確切的發病率不明,因為疑似病例不常經由組織學檢查 (histologic examination) 證實。LP 可與 LS 並存,這可能可解釋部分口腔病灶。LS 與 morphea 並存也曾被記錄。曾有一例
- 此病在女性極為罕見。
組織學特徵 (Histologic Features)
- 組織學具特徵性,且與其他部位的 porokeratosis 相同。在 porokeratosis ptychotropica 中,多數病例疊加有苔癬化 (lichenification) 的變化,使 cornoid lamella 模糊不清。後者加上斜向切片 (oblique sectioning) 意味著,除非有高度懷疑並進行進一步切片,否則此病可能被遺漏。
- 曾有報導一例接受 imatinib mesylate 治療之病人出現多發性生殖器與生殖器外病灶。另有一例與異體幹細胞移植 (allogeneic stem cell transplantation) 相關,以及另一例在男變女性別重置 (male-to-female gender reassignment) 病例所使用的陰囊皮膚 (scrotal skin) 上發生生殖器疾病,皆有記錄。
- LS 的典型病灶為瓷白色丘疹與斑塊 (porcelain-white papules and plaques),表面有皺褶 (crinkled surface)。它們可融合形成斑塊。常伴隨瘀斑 (ecchymoses) 與角化過度區 (areas of hyperkeratosis)。後者發生於附屬器開口 (appendage ostia) 處,其呈擴張狀,產生稱為 delling 的物理徵象。水疱 (Bullae) 僅罕見發生。
- 女性常見症狀包括搔癢 (pruritus)、灼熱感 (burning) 與性交疼痛 (dyspareunia),在男性則為性交與排尿困難 (coital and urinary difficulties)。雖然肛門生殖器 LS 極度搔癢,苔癬化常不明顯。
- 女性肛門生殖器受累典型為對稱性且雙側性 (symmetrical and bilateral),當同時侵犯肛周與外陰皮膚時,被描述為呈八字形(沙漏狀)分布 (figure-of-eight [hourglass] distribution)。
- 在男性,受累呈「鬱金香樣」(tulip-like),對稱性侵犯陰莖遠端體部、龜頭與包皮 (distal penile shaft, glans, and foreskin)(不侵犯肛周皮膚)(Fig. 12.52)。另一方面,表現也可能為完全性包莖 (complete phimosis) (Fig. 12.53)。
- 外陰 (vulva) 上的病灶主要侵犯大陰唇內側面 (inner aspect of the labia majora)、小陰唇 (labia minora)、陰蒂包皮 (prepuce of the clitoris)、舟狀窩 (fossa navicularis) 與後聯合 (posterior commissure) (Figs 12.54 and 12.55)。陰莖疾病可侵犯龜頭與遠端包皮,繫帶 (frenulum) 與腹側冠下溝 (ventral subcoronal sulcus) 是特別的目標。發炎可為苔癬樣 (lichenoid) 與 Zoon 樣 (Zoonoid)。
- LS 是一種瘢痕性疾病 (scarring disorder),在女性可能有顯著的解剖學變化,包括小陰唇吸收 (resorption of the labia minora)、陰蒂埋沒 (burying of the clitoris) 與陰道口狹窄 (introital narrowing)。陰道 (vagina) 不受影響。尿道受累 (Urethral involvement) 極為罕見。
- 在男性可能有完全性包莖、因硬化帶 (sclerotic band) 所致的緊縮性包皮炎 (constrictive posthitis)(「束腰」(waisting))、跨冠與冠下沾黏 (transcoronal and subcoronal adhesions)、繫帶的糜爛、潰瘍與破壞或閉塞、冠狀溝結構與輪廓的消失(例如珍珠樣陰莖丘疹 (pearly penile papules) 的喪失),以及尿道口「針孔」狹窄 (meatal ‘pin hole’ narrowing)。前尿道 (anterior urethra) 的受累可能很嚴重:因尿道狹窄 (urethral stricture) 接受尿道成形術 (urethroplasty) 的病人中,有 29% 具有 LS 的病理證據。
- genital LS 的一個重要併發症是發育不良 (dysplasia) 與 SCC 的發生。後者僅極例外地被報導與生殖器外病灶相關。在外陰 (Figs 12.56 and 12.57),發育不良灶 (dysplastic foci) 可表現為角化過度黏附性灰白色區域 (hyperkeratotic adherent, gray-white areas)、冰錐狀糜爛 (ice pick erosions) 或固定性紅斑區 (fixed areas of erythema)。此類變化必須經組織學檢查。患有 vulval LS 的病人中,少於 4% 會發生 SCC。
- 近期顯示,診斷為 LS 並進展為 SCC 的相當數量病例,實際上代表分化型外陰上皮內瘤變 (differentiated vulvar intraepithelial neoplasia) 而非 LS。誤診病例數量高的主要原因,可能在於以組織學標準診斷分化型外陰瘤變的困難。這些病人傾向於更快速地進展為侵襲性 SCC。在真正 LS 並進展的這組病人中,可見一些在無進展病例中不存在的組織學特徵。有人建議這些標準可用以辨識高風險病人,它們包括角化不全 (parakeratosis)、角化不良 (dyskeratosis)、增生 (hyperplasia) 與基底細胞非典型性 (basal cell atypia)。
- 在男性,已發表的 LS 併發 SCC 之風險介於 4% 與 8% 之間。當檢查陰莖 SCC 的切除標本時,在 32% 至 50% 的病例中發現 LS。與 LS 相關的陰莖 SCC 類型通常不與 HPV 相關。慢性病程、不對稱性、紅斑、Zoon 樣或紅斑增生病 (erythroplasia)、糜爛、潰瘍與疣狀變化都必須以極高度的懷疑看待,並以低門檻進行切片。
- 病例已被充分認識,並曾在兩性中以及在同卵與異卵雙胞胎 (identical and nonidentical twins) 中被描述。近期一項研究發現高達 12% 的病人有家族史,提示一部分病例具有遺傳成分 (genetic component)。約 21% 的 LS 病人有相關的自體免疫疾病 (autoimmune disease),包括圓禿 (alopecia areata)、白斑 (vitiligo)、甲狀腺機能亢進 (hyperthyroidism)、甲狀腺機能低下 (hypothyroidism)、惡性貧血 (pernicious anemia) 與糖尿病 (diabetes mellitus)。
- 病人及其一等親 (first-degree relatives) 可能有循環自體抗體 (circulating autoantibodies),包括抗甲狀腺、抗胃壁細胞 (gastric parietal cell) 與抗平滑肌 (smooth muscle) 抗體,以及抗核因子 (antinuclear factor)。曾有報導 LS 與第 II 類抗原 (class II antigens) 的存在之間有顯著相關,包括 HLA-DQ7、-DR7、-DQ8 與 -DQ9(單獨或合併)。也有人提出 HLA-A2 可能發揮保護作用,因為它傾向於在具有廣泛生殖器外病灶的病人中缺失。此外,HLA-DR4 與 -DQ8 的連鎖在肛門生殖器區有顯著結構性損害的病人中更為常見。
- 在患有 genital LS 的男性與女性血清中,曾發現對醣蛋白細胞外基質蛋白 1 (glycoprotein extracellular matrix protein 1) 的循環 IgG 抗體。在少數其他方面健康、患有 vulval LS 的兒童中,曾偵測到對 BP180 抗原的 IgG 自體抗體。
- 曾有與 LS 相關之非典型黑色素細胞病灶 (atypical melanocytic lesions) 的報導,需要仔細的臨床病理對照 (clinicopathological correlation)。也有 melanoma 於 LS 中發生的病例報導。
致病機轉與組織學特徵 (Pathogenesis and Histologic Features)
- LS 的病因尚無共識。有人提出遺傳 (genetic)、荷爾蒙 (hormonal) 與自體免疫 (autoimmune) 因素可能具重要性。家族性
- 有趣的是,genital LS 曾被報導發生於骨髓移植 (bone marrow transplant) 受贈者與移植物抗宿主病 (graft-versus-host disease) 中。
- 與一般人群相比,患有 genital LS 的女性被發現有較高的 psoriasis 發生率(主要為生殖器外)。
- 停經前女性發生的 LS 曾被連結到口服避孕藥 (oral contraceptives) 的使用,特別是具有抗雄激素 (antiandrogenic) 特性者。
- 其他提出的病因因素包括膠原酶 (collagenase) 缺乏、膠原抑制酶 (collagen inhibitor enzyme) 增加,以及彈性蛋白酶 (elastase) 活性降低。曾有描述部分病人雙氫睪固酮 (dihydrotestosterone) 濃度降低,並有一篇報導記載組織學上可變抗酸桿菌 (variably acid-fast bacilli) 的存在。
- 如同 morphea 與 atrophoderma,曾有人提出與 Borrelia burgdorferi 的因果關係,但此推測性連結源自歐洲 (Europe) 而非美國 (United States) 的病例。
- 在英國患有 genital LS 的男性中,並無與 Borrelia 相關的血清學證據。Borrelia 僅例外地透過巢式聚合酶連鎖反應 (nested polymerase chain reaction, PCR) 在 LS 中被證實。結果不一致可能是由於偵測 Borrelia 所用的技術,並有人建議聚焦浮動顯微術 (focus floating microscopy) 應作為偵測的金標準 (gold standard)。
- 在一項研究中,HPV(型別 6、16 與 18)在 70% 的兒童期陰莖 LS 病例與 17.4% 的成人病例(型別 16、18、45)中被報導,相較之下正常男性為 8.7%;在另一項研究中於 33% 的成人病例(型別 16、18、33、51)被報導。LS 的局部類固醇治療 (Topical steroid treatment) 可能導致 HPV 再活化。然而,在其他 vulval LS 的研究中並未發現 HPV。在同一項研究中,EB 病毒 (Epstein–Barr virus, EBV) 在 26.5% 的樣本中被報導。然而,LS 的流行病學與臨床特性並非感染性或性傳播疾病 (sexually transmitted disease) 的特性。
- 在男性,肥胖 (obesity)、解剖學異常 (anatomical abnormality) 與創傷 (trauma) 似乎是促成因素。LS 曾被特別連結到尿道下裂 (hypospadias) 及其修補手術。它常見於尿路造口 (urostomies) 與尿道造口 (urethrostomies) 周圍。在某百分比的軟纖維瘤 (acrochordons, skin tags) 中存在 LS 的組織病理特徵,這引出鬆弛皮膚封閉 (occlusion of flaccid skin) 為致病因子的提示。至少在男性,所有證據都指向 LS 是由於與尿液 (urine) 慢性間歇性封閉接觸所致,此接觸繼發於尿液微失禁 (urinary microincontinence)。

圖 12-48:Lichen sclerosus:青春期前疾病,顯示大陰唇上部的蒼白 (pallor) 與肛周病灶 (perianal lesions)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.48 Lichen sclerosus: prepubertal disease showing pallor on upper labia majora and perianal lesions. By courtesy of the Institute of Dermatology, London, UK.

圖 12-49:Lichen sclerosus:肛周疾病 (perianal disease) 常與外陰受累一併存在,形成所謂的沙漏狀分布 (hourglass distribution)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.49 Lichen sclerosus: perianal disease is often present in addition to vulval involvement, giving rise to the so-called hourglass distribution. By courtesy of the Institute of Dermatology, London, UK.

圖 12-50:Lichen sclerosus:不規則白色斑塊 (irregular white plaque)。應注意生殖器外病灶有時在無生殖器病灶的情況下發生。由 R.A. Marsden, MD, St George’s Hospital, London, UK 提供。
Fig. 12.50 Lichen sclerosus: irregular white plaque. It should be noted that extragenital lesions sometimes occur in the absence of genital lesions. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 12-51:Lichen sclerosus:癒合中的病灶,呈典型「皺褶薄紙樣」(wrinkled tissue paper) 外觀。由 R.A. Marsden, MD, St George’s Hospital, London, UK 提供。
Fig. 12.51 Lichen sclerosus: healing lesion with a typical ‘wrinkled tissue paper’ appearance. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

圖 12-52:Lichen sclerosus:在男性,包皮與龜頭的病灶可能併發尿道狹窄 (urethral stricture)(所謂的 balanitis xerotica obliterans)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.52 Lichen sclerosus: in males, lesions of the foreskin and glans may be complicated by urethral stricture (so-called balanitis xerotica obliterans). By courtesy of the Institute of Dermatology, London, UK.

圖 12-53:Lichen sclerosus:較進展的病例,顯示嚴重包莖 (severe phimosis)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.53 Lichen sclerosus: a more advanced case showing severe phimosis. By courtesy of the Institute of Dermatology, London, UK.

圖 12-54:Lichen sclerosus:對稱性白色病灶,伴有重度萎縮 (gross atrophy) 與出血 (hemorrhage)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.54 Lichen sclerosus: symmetrical white lesions with gross atrophy and hemorrhage. By courtesy of the Institute of Dermatology, London, UK.

圖 12-55:Lichen sclerosus:有廣泛的外陰疾病 (vulval disease),併會陰 (perineum) 受累與萎縮。由 Institute of Dermatology, London, UK 提供。
Fig. 12.55 Lichen sclerosus: there is extensive vulval disease with involvement of the perineum and atrophy. By courtesy of the Institute of Dermatology, London, UK.

圖 12-56:Lichen sclerosus:長期存在的疾病,伴外陰結構完全喪失 (complete loss of the vulval architecture),併發潰瘍性鱗狀細胞癌 (ulcerated squamous cell carcinoma)。由 Institute of Dermatology, London, UK 提供。
Fig. 12.56 Lichen sclerosus: long-standing disease with complete loss of the vulval architecture complicated by the development of an ulcerated squamous cell carcinoma. By courtesy of the Institute of Dermatology, London, UK.
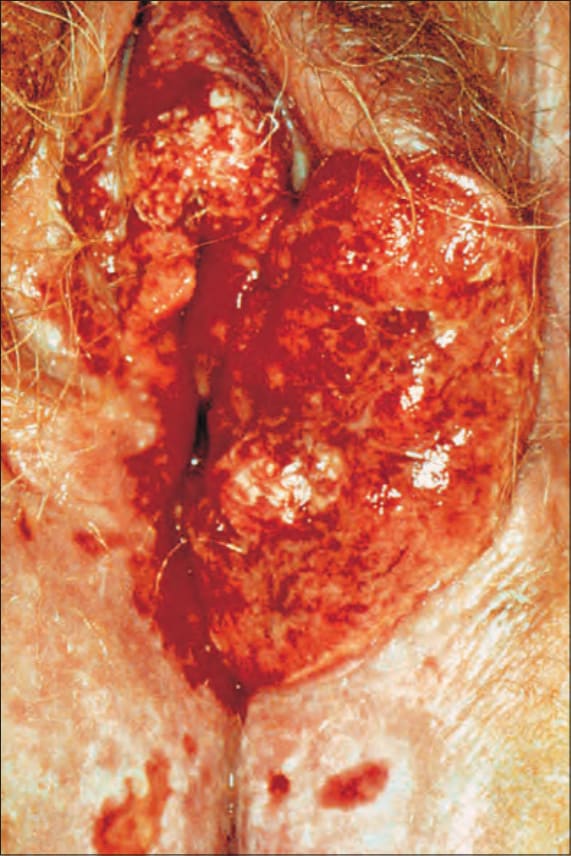
圖 12-57:Lichen sclerosus:一個潰瘍性鱗狀細胞癌已破壞外陰左側大部分。注意背景的潰瘍性 lichen sclerosus。由 Institute of Dermatology, London, UK 提供。
Fig. 12.57 Lichen sclerosus: an ulcerated squamous cell carcinoma has destroyed much of the left side of the vulva. Note the background of ulcerated lichen sclerosus. By courtesy of the Institute of Dermatology, London, UK.
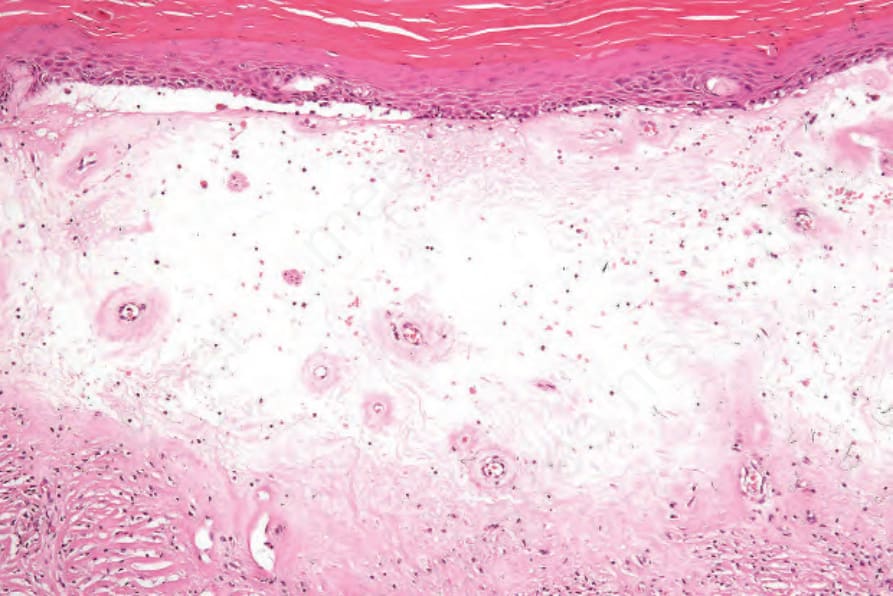
圖 12-59:Lichen sclerosus:此例顯示 lichen sclerosus 的特徵性表現。注意角化過度 (hyperkeratosis)、表皮萎縮 (epidermal atrophy) 與一條寬的真皮玻璃樣變帶 (broad band of dermal hyalinization)。微血管擴張血管 (Telangiectatic vessels) 顯著。
Fig. 12.59 Lichen sclerosus: this example shows the characteristic features of lichen sclerosus. Note the hyperkeratosis, epidermal atrophy, and a broad band of dermal hyalinization. Telangiectatic vessels are prominent.
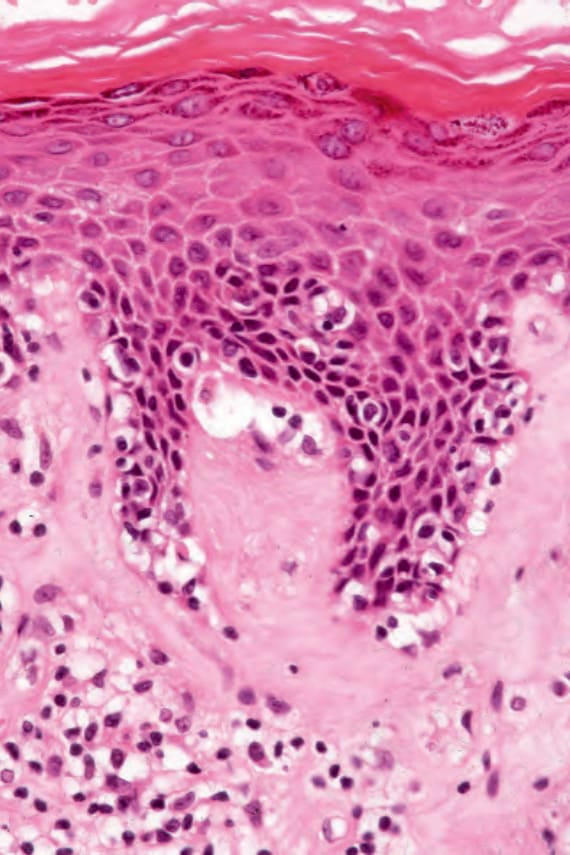
圖 12-60:Lichen sclerosus:基底細胞水腫變性 (basal cell hydropic degeneration) 的近觀。
Fig. 12.60 Lichen sclerosus: close-up view of basal cell hydropic degeneration.
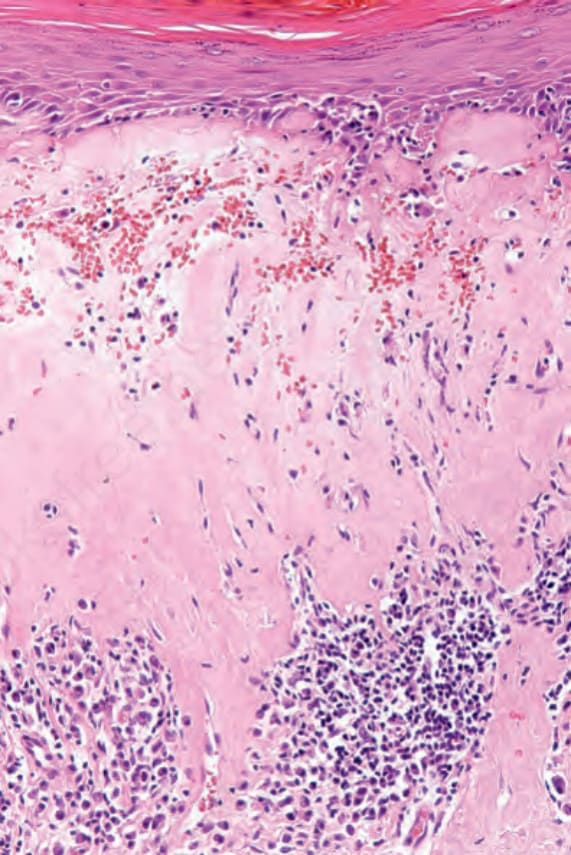
圖 12-61:Lichen sclerosus:在此視野中,淋巴組織球性浸潤 (lymphohistiocytic infiltrate) 位於玻璃樣變帶 (zone of hyalinization) 深處。有微血管擴張 (telangiectasia) 併出血。
Fig. 12.61 Lichen sclerosus: in this view, the lymphohistiocytic infiltrate is present deep to the zone of hyalinization. There is telangiectasia with hemorrhage.

圖 12-63:Zoon balanitis:有龜頭、包皮與陰莖體部 (glans, prepuce, and shaft of the penis) 的受累。取自 Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.
Fig. 12.63 Zoon balanitis: there is involvement of the glans, prepuce, and shaft of the penis. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.
- 無論受累部位為何,組織學變化皆相同 (Figs 12.58–12.61)。然而,生殖器病灶相較於發生在生殖器外部位者,常顯示無萎縮 (absence of atrophy)、慢性單純苔癬樣變化 (lichen simplex chronicus-like changes)、海綿水腫 (spongiosis)、較常見的血管擴張 (vascular ectasia) 與真皮嗜酸性球 (dermal eosinophils)。
- 另一方面,extragenital LS 在許多病例中似乎與彈性纖維吞噬作用 (elastophagocytosis) 相關,此特徵在 genital LS 中未被報導。偶爾,在無假性黃色瘤彈性纖維 (pseudoxanthoma elasticum) 的病人中可見假性黃色瘤彈性纖維樣纖維 (pseudoxanthoma elasticum-like fibers)。
- 完全發展的 LS 病灶顯示變薄、消平的表皮 (thinned, effaced epidermis),伴介面變化 (interface change),以及上真皮的一條寬玻璃樣變帶 (wide band of hyalinization),於玻璃樣變區下方有淋巴組織球性浸潤 (lymphohistiocytic infiltrate)。Zoon 樣發炎 (Zoonoid inflammation) 可能顯著。常見明顯的角化過度 (hyperkeratosis),於有毛皮膚常伴隨毛囊栓塞 (follicular plugging)。
- 有時存在表皮下水腫 (Subepidermal edema),並可能足以造成上皮下水疱 (subepithelial vesiculation) (Fig. 12.62)。微血管擴張 (Telangiectasia) 常見,紫斑 (purpura) 可為額外特徵。也可發展出血管角皮瘤樣病灶 (Angiokeratoma-like lesions)。一個類似的現象是淋巴管擴張 (lymphangiectasia)。
- 早期病灶與完全發展病灶的邊緣顯示類似 LP 的苔癬樣變化(見鑑別診斷)。部分病例可能與明顯且高度不規則的棘層肥厚 (acanthosis) 灶相關,常具有非常鋸齒狀的下緣(所謂的鱗狀細胞增生 (squamous cell hyperplasia))。此類病例應仔細審視是否有上皮發育不良 (epithelial dysplasia)(分化型上皮內瘤變 (differentiated intraepithelial neoplasia))或鄰近癌 (adjacent carcinoma) 的證據。分化型上皮內瘤變是在與 LS 相關的 SCC 中發現的、目前為止最常見的
- 發育不良類型。目前無證據提示致癌性 HPV (oncogenic HPV) 與 LS 相關性 SCC 相關。
- 在 LS 中偶爾觀察到動脈內膜炎 (endarteritis),最初導致了「obliterans」一詞的使用。在兩例男孩中,發現真皮淋巴組織球性與肉芽腫性靜脈炎 (granulomatous phlebitis),其中一例也有 HPV 的證據。曾有一例罕見的 LS 伴相關嗜酸性海綿水腫 (eosinophilic spongiosis),代表疊加的大疱性類天疱瘡 (bullous pemphigoid) 之報導。
- LS 的超微結構研究 (Ultrastructural studies) 顯示基底膜板 (basal lamina) 的片段化 (fragmentation)、重複 (reduplication) 與間隙形成 (formation of gaps)。Langerhans 細胞 (Langerhans cells) 似乎穿過這些間隙。LS 中的單核細胞浸潤由輔助型 (T-helper) 與抑制型淋巴球 (suppressor lymphocytes) 的混合所組成。LS 中曾報導表皮細胞表現 p53。後者較常見於與 SCC 相關的病例。
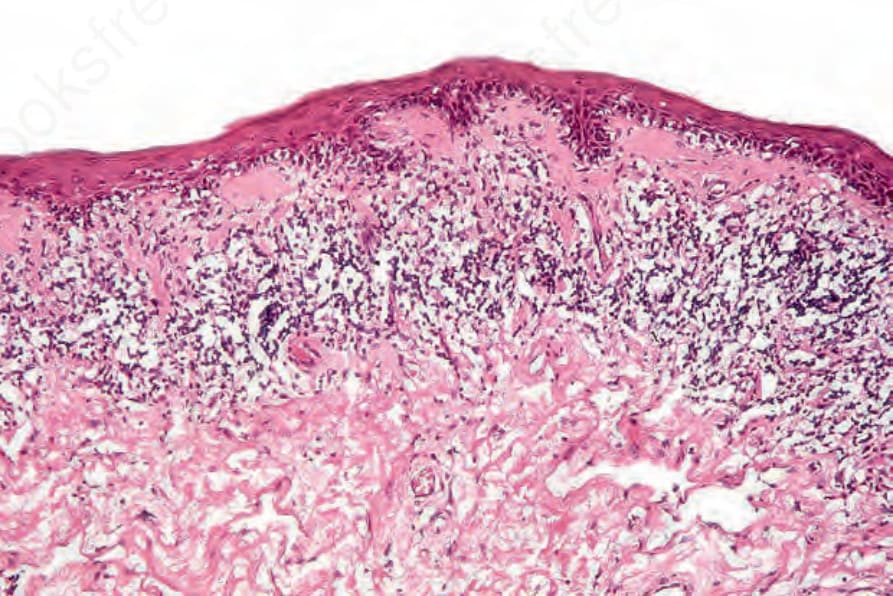
圖 12-58:Lichen sclerosus:早期病灶,顯示表皮萎縮 (epidermal atrophy) 與明顯的基底細胞水腫變性 (basal cell hydropic degeneration)。有一狹窄的乳頭層真皮玻璃樣變區 (papillary dermal hyalinization),並存在帶狀浸潤 (bandlike infiltrate)。
Fig. 12.58 Lichen sclerosus: early lesion showing epidermal atrophy and marked basal cell hydropic degeneration. There is a narrow zone of papillary dermal hyalinization and a bandlike infiltrate is present.
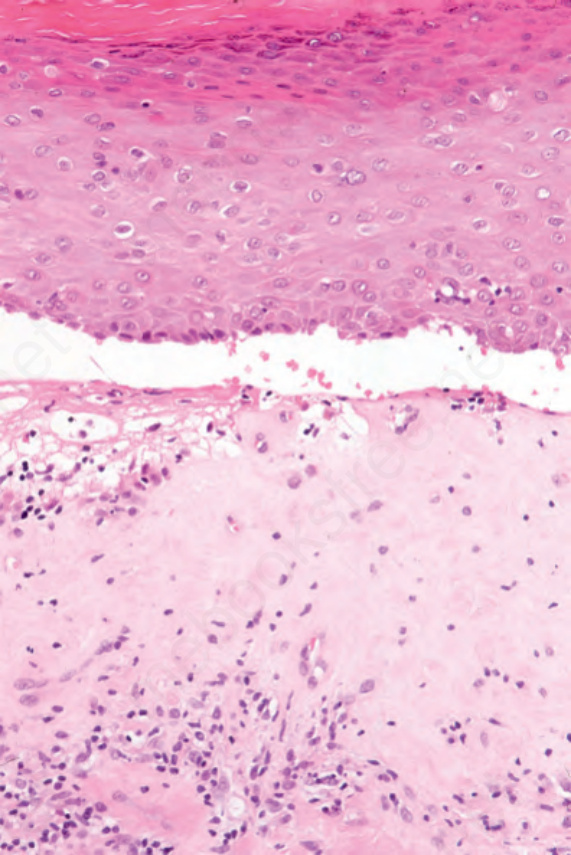
圖 12-62:Lichen sclerosus:偶爾,劇烈水腫可導致表皮下水疱 (subepidermal vesiculation)。
Fig. 12.62 Lichen sclerosus: occasionally, intense edema may result in subepidermal vesiculation.