Porokeratosis
Porokeratosis
Clinical features Typical annular lesions with a raised hyperkeratotic margin (see Chapter
3) are classically generalized in distribution but the anogenital skin may be involved. Rarely, the genital skin is affected alone (genital porokeratosis) or, even more rarely, pruritic, occasionally verrucous involvement limited to the perianal and gluteal folds is seen (porokeratosis ptychotropica).1–3 The differential diagnosis includes LP and amyloid (and the latter has been reported in porokeratosis ptychotropica).4 An association with bone marrow transplantation has been described.3
There are two peaks of incidence; in females these occur in the prepubertal years and then post-menopause, and in males in prepubertal and young to middle-aged adult males. When the disease arises in childhood it tends to persist, regression being uncommon.3 In girls, the condition can present at a very early age with hemorrhagic perianal lesions (Figs 12.48 and 12.49. Constipation can occur as a complication of the painful fissuring of the anal canal. If there is marked anogenital involvement, the condition may be mistaken for sexual abuse.4 Perianal disease does not occur in males, but in boys, genital LS is the most common cause of phimosis. Extragenital lesions occur in 11% of women with genital LS.5 Such involvement occurs on the upper trunk, groins, upper extremities, neck, lower trunk, and lower extremities in decreasing order of frequency, often at sites of friction (Figs 12.50 and 12.51). Involvement of the scalp and face is rare and can be associated with alopecia.6–8 An exceptional case with plantar involvement has been documented.9 It is very rare to see extragenital lesions in the absence of genital lesions. The Koebner phenomenon is frequent and LS has been described in association with scars, at the sites of radiotherapy, and insulin injection and in association with a tattoo.10–13 Lesions can also develop or recur in skin or myocutaneous grafts.14 Oral involvement including lip lesions as an isolated phenomenon or in association with genital lesions has been described.15–17 The exact incidence of the latter is unknown, as suspected cases are not often confirmed by histologic examination.18 LP can coexist with LS, and this may account for some of the oral lesions.19 Coexistence of LS with morphea has also been documented.20 A single case
The condition is exceptionally rare in females.5
Histologic features The histology is distinctive and the same as porokeratosis at other sites. In porokeratosis ptychotropica, most cases have superimposed changes of lichenification which obscures the cornoid lamella. The latter and oblique sectioning means that the condition may be missed unless there is a high index of suspicion and further sections are performed.
487 Inflammatory dermatoses
of multiple genital and extragenital lesions in a patient receiving imatinib mesylate has been reported.21 A further case in association with allogeneic stem cell transplantation and another of genital disease developing in scrotal skin used in a case of male-to-female gender reassignment have been documented.22,23
The typical lesions of LS are porcelain-white papules and plaques with a crinkled surface. They can coalesce to form plaques. There are often associated ecchymoses and areas of hyperkeratosis. The latter occurs in relation to the appendage ostia, which are dilated, giving rise to the physical sign of delling. Bullae only rarely occur. Common symptoms in women include pruritus, burning, and dyspareunia, and in men coital and urinary difficulties. Although anogenital LS is intensely pruritic, lichenification is often not conspicuous. Female anogenital involvement is typically symmetrical and bilateral, and is described as having a figure-of-eight (hourglass) distribution when it affects the perianal as well as vulval skin. In men the involvement is ‘tulip-like’ symmetrically affecting the distal penile shaft, glans, and foreskin (not the perianal skin) (Fig. 12.52). On the other hand, the presentation may be with complete phimosis (Fig. 12.53). Lesions on the vulva predominantly affect the inner aspect of the labia majora, the labia minora, the prepuce of the clitoris, the fossa navicularis, and the posterior commissure (Figs 12.54 and 12.55). Penile disease can affect the glans, and distal foreskin, the frenulum, and ventral subcoronal sulcus is a particular target. Inflammation can be lichenoid and Zoonoid. LS is a scarring disorder, and in women there may be marked anatomical changes with resorption of the labia minora, burying of the clitoris, and introital narrowing. The vagina is unaffected. Urethral involvement is very rare.24 In men there may be complete phimosis, constrictive posthitis due to a sclerotic band (‘waisting’), transcoronal and subcoronal adhesions, erosion, ulceration and destruction or obliteration of the frenulum, effacement of the coronal sulcal architecture and definition (e.g., loss of pearly penile papules), and meatal ‘pin hole’ narrowing. The involvement of the anterior urethra can be serious: 29% of patients undergoing urethroplasty for urethral stricture had pathological evidence of LS.
An important complication of genital LS is the development of dysplasia and SCC. The latter only very exceptionally has been reported in association with extragenital lesions.25 In the vulva (Figs 12.56 and 12.57), dysplastic foci may appear as hyperkeratotic adherent, gray-white areas, ice pick erosions, or fixed areas of erythema. Such changes must be examined histologically. Less than 4% of patients with vulval LS will develop an SCC.26 It has recently been shown that an important number of cases diagnosed as LS
with progression to SCC actually represent differentiated vulvar intraepithelial neoplasia and not LS.27 The main reason for the high number of misdiagnosed cases is probably the difficulty in diagnosing differentiated vulval neoplasia on histologic grounds. These patients tend to have a more rapid progression to invasive SCC. In the group of patients with true LS and progression, a number of histologic features are seen which are absent in cases without progression. It has been suggested that these criteria can be used to identify patients at risk. They include parakeratosis, dyskeratosis, hyperplasia, and basal cell atypia.27 In males, the published risk of SCC complicating LS is between 4% and 8%.28–31 When excision specimens of penile SCC are examined, LS has been found in between 32% and 50% of cases.31–33 The type of penile SCC associated with LS is not usually associated with HPV.34 Chronicity, asymmetry, erythema, zoonoid or erythroplasia, erosions, ulcers, and verrucous change must be regarded with a very high index of suspicion and a low threshold for biopsy.
488 Diseases of the anogenital skin
cases are well recognized and have been described in both sexes and in identical and nonidentical twins.39–42 A recent study found a family history in up to 12% of patients, suggesting that a number of cases have a genetic component.43 About 21% of patients with LS have an associated autoimmune disease including alopecia areata, vitiligo, hyperthyroidism, hypothyroidism, pernicious anemia, and diabetes mellitus.44,45 Patients and first-degree relatives may have circulating autoantibodies including those to thyroid, gastric parietal cell, and smooth muscle in addition to antinuclear factor.46 A significant association between LS and the presence of class II antigens including HLA-DQ7, -DR7, -DQ8, and -DQ9 (alone or in combination) has been reported.47 It has also been suggested that HLA-A2 possibly exerts a protective role, as it tends to be absent in patients with extensive extragenital lesions. Also, linkage of HLA-DR4 with -DQ8 is more common in patients with marked structural damage to the anogenital area. Circulating IgG antibodies to the glycoprotein extracellular matrix protein 1 have been found in the sera of men and women with genital LS.48,49 In a few otherwise healthy children with vulval LS, IgG autoantibodies against the BP180 antigen have been detected.50
There are reports of atypical melanocytic lesions in association with LS,35,36 and careful clinicopathological correlation is needed. Cases of melanoma developing in LS are also reported.37,38
Pathogenesis and histologic features The etiology of LS is not consensually agreed. It has been suggested that genetic, hormonal, and autoimmune factors may be of importance. Familial
Intriguingly, genital LS has been reported in bone marrow transplant recipients and graft-versus-host disease.51,52
Women with genital LS have been found to have a higher incidence of psoriasis (predominantly extragenital) compared with the general population.53,54
LS developing in premenopausal women has been linked to the use of oral contraceptives, particularly those with antiandrogenic properties.55
Additional proposed etiological factors include absence of collagenase, an increase in collagen inhibitor enzyme, and decreased elastase activity. Reduced dihydrotestosterone levels have been described in some patients and there is one report documenting the histologic presence of variably acid-fast bacilli.56,57 As with morphea and atrophoderma, a causal relationship to Borrelia burgdorferi has been proposed, but this putative connection derives from cases in Europe and not the United States.58 There is no serological evidence in British men with genital LS for an association with
489 Inflammatory dermatoses
Borrelia.59 Borrelia has only exceptionally been demonstrated by nested polymerase chain reaction (PCR) in LS.60 The variable results may be due to techniques used to detect Borrelia, and it has been suggested that focus floating microscopy should be the gold standard for detection.61 HPV (types 6, 16, and 18) has been reported in 70% of cases of childhood penile LS and in 17.4% of adult cases (types 16, 18, 45) compared with 8.7% of normal males in one study and in 33% of adult cases (types 16, 18, 33, 51) in another.52–64 Topical steroid treatment of LS may lead to HPV reactivation.65 HPV, however, has not been found in other studies of vulval LS.66 Epstein–Barr virus (EBV) was reported in 26.5% of samples in the same study. However, the epidemiology and clinical tenor of LS is not that of an infectious or sexually transmitted disease.
In males, obesity, anatomical abnormality, and trauma seem to be contributing factors.2,24,67 LS has been specifically related to hypospadias and its repair.24,68 It is often found around urostomies and urethrostomies.69 The presence of histopathological features of LS in a percentage of acrochordons (skin tags) has led to the suggestion that occlusion of flaccid skin is a pathogenic factor.70 In men, at least, all the evidence points to LS being due to chronic intermittent occluded contact with urine consequent upon contact with urinary microincontinence.71

Fig. 12.48 Lichen sclerosus: prepubertal disease showing pallor on upper labia majora and perianal lesions. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.49 Lichen sclerosus: perianal disease is often present in addition to vulval involvement, giving rise to the so-called hourglass distribution. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.50 Lichen sclerosus: irregular white plaque. It should be noted that extragenital lesions sometimes occur in the absence of genital lesions. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 12.51 Lichen sclerosus: healing lesion with a typical ‘wrinkled tissue paper’ appearance. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.

Fig. 12.52 Lichen sclerosus: in males, lesions of the foreskin and glans may be complicated by urethral stricture (so-called balanitis xerotica obliterans). By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.53 Lichen sclerosus: a more advanced case showing severe phimosis. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.54 Lichen sclerosus: symmetrical white lesions with gross atrophy and hemorrhage. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.55 Lichen sclerosus: there is extensive vulval disease with involvement of the perineum and atrophy. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.56 Lichen sclerosus: long-standing disease with complete loss of the vulval architecture complicated by the development of an ulcerated squamous cell carcinoma. By courtesy of the Institute of Dermatology, London, UK.
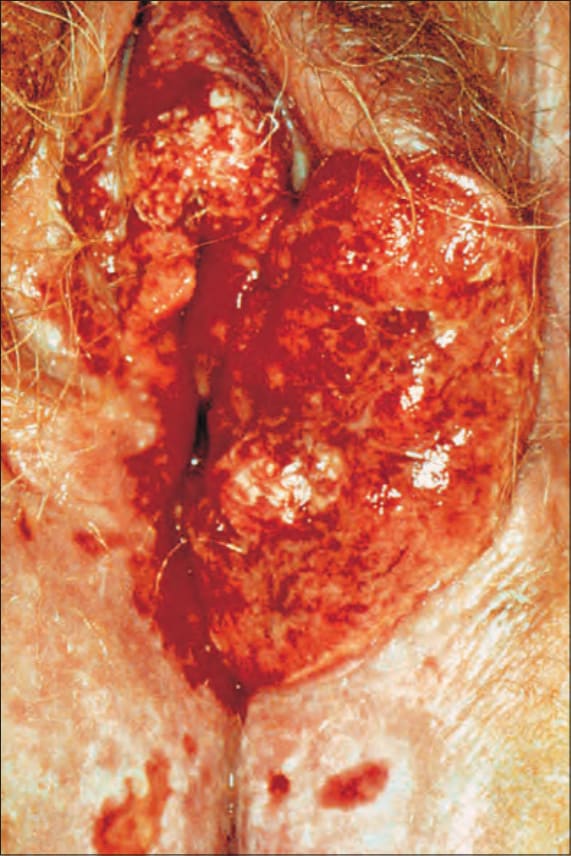
Fig. 12.57 Lichen sclerosus: an ulcerated squamous cell carcinoma has destroyed much of the left side of the vulva. Note the background of ulcerated lichen sclerosus. By courtesy of the Institute of Dermatology, London, UK.
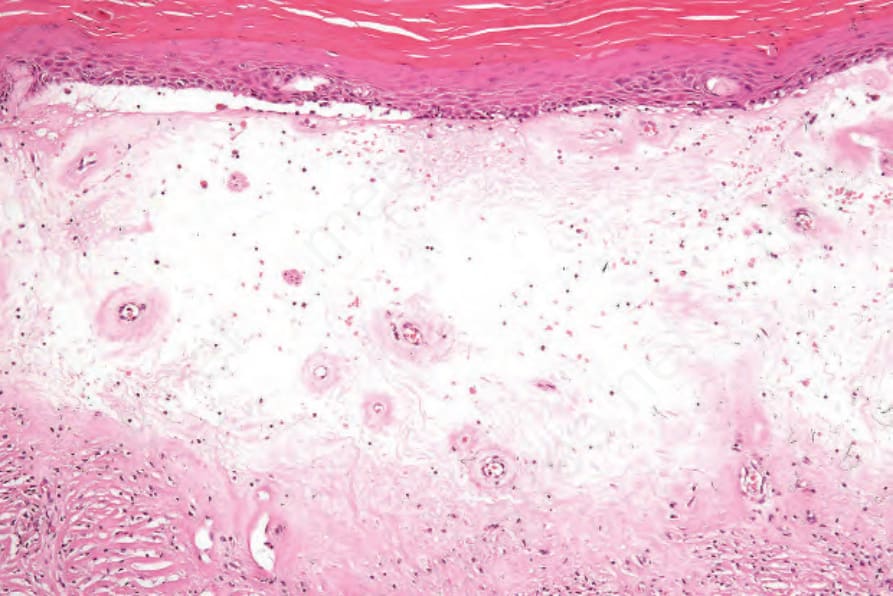
Fig. 12.59 Lichen sclerosus: this example shows the characteristic features of lichen sclerosus. Note the hyperkeratosis, epidermal atrophy, and a broad band of dermal hyalinization. Telangiectatic vessels are prominent.
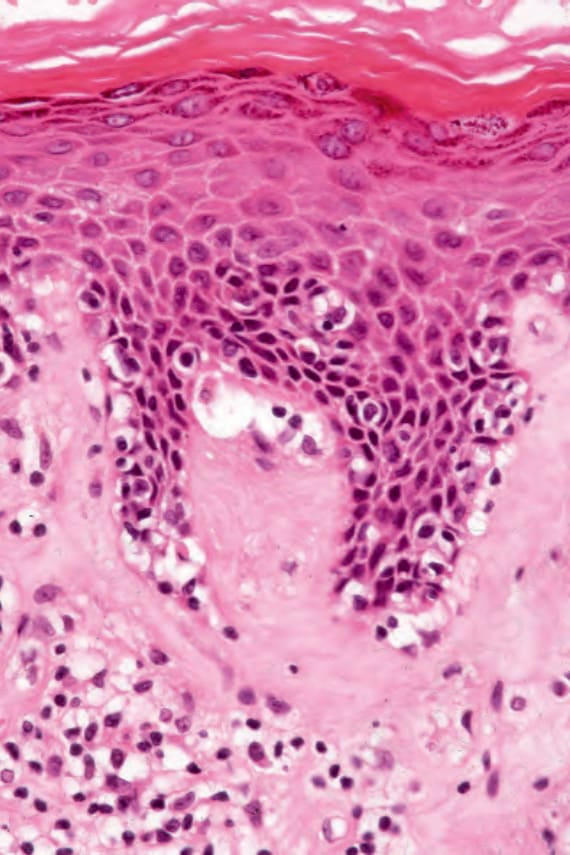
Fig. 12.60 Lichen sclerosus: close-up view of basal cell hydropic degeneration.
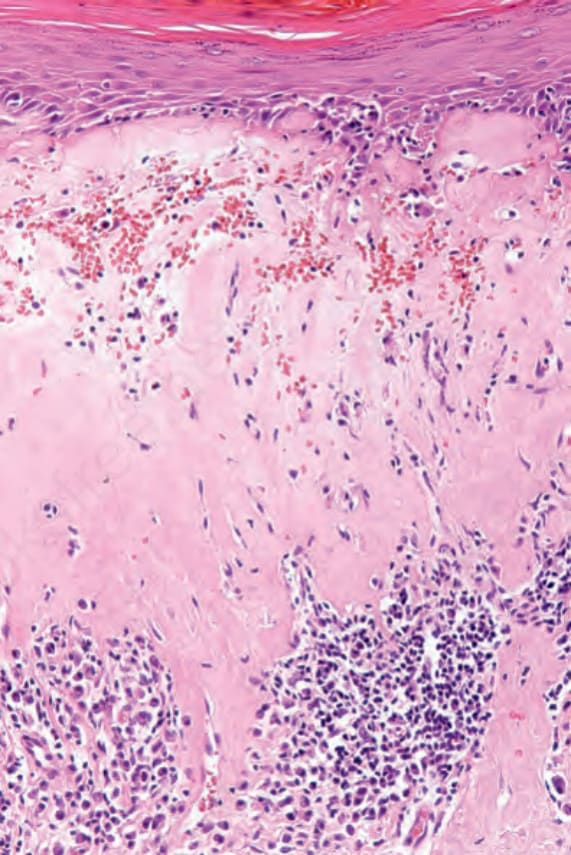
Fig. 12.61 Lichen sclerosus: in this view, the lymphohistiocytic infiltrate is present deep to the zone of hyalinization. There is telangiectasia with hemorrhage.

Fig. 12.63 Zoon balanitis: there is involvement of the glans, prepuce, and shaft of the penis. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.
The histologic changes are identical irrespective of the site involved (Figs 12.58–12.61).72–74 However, genital lesions, as opposed to those occurring at extragenital sites, often show absence of atrophy, lichen simplex chronicus-like changes, spongiosis, more prevalent vascular ectasia, and dermal eosinophils.75,76 Extragenital LS, on the other hand, seems to be associated in a number of cases with elastophagocytosis, a feature not reported in genital LS.77 Occasionally, pseudoxanthoma elasticum-like fibers may be seen in patients without pseudoxanthoma elasticum.78 Fully developed lesions of LS show a thinned, effaced epidermis with interface change and a wide band of hyalinization in the upper dermis and a lymphohistiocytic infiltrate below the hyalinized area. Zoonoid inflammation may be prominent. Marked hyperkeratosis, often associated with follicular plugging on hair-bearing skin, is frequently seen. Subepidermal edema is sometimes present and may be sufficient to cause subepithelial vesiculation (Fig. 12.62). Telangiectasia is common and purpura may be an additional feature. Angiokeratoma-like lesions can also develop.79 A similar phenomenon is that of lymphangiectasia.80 Early lesions and the periphery of fully developed lesions display lichenoid changes similar to LP (see differential diagnosis). Some cases may be associated with foci of marked and highly irregular acanthosis, often with a very jagged lower border (so-called squamous cell hyperplasia). Such cases should be carefully scrutinized for evidence of epithelial dysplasia (differentiated intraepithelial neoplasia) or adjacent carcinoma. Differentiated intraepithelial neoplasia is by far the most common
type of dysplasia found in SCC associated with LS.81 Currently, there is no evidence to suggest that oncogenic HPV is associated with LS-related SCC.
The occasional observation of endarteritis in LS led originally to the usage of the term ‘obliterans’. In two cases in boys, a dermal lymphohistiocytic and granulomatous phlebitis was found, and one also had evidence of HPV.82 An exceptional case of LS with associated eosinophilic spongiosis representing superimposed bullous pemphigoid has been reported.83
Ultrastructural studies of LS show fragmentation, reduplication, and formation of gaps in the basal lamina.75,84 Langerhans cells appear to pass through these gaps. The mononuclear infiltrate in LS is composed of an admixture of T-helper and suppressor lymphocytes. Expression of p53 by epidermal cells has been reported in LS.76,85 The latter is more often seen in cases associated with SCC.86
490 Diseases of the anogenital skin
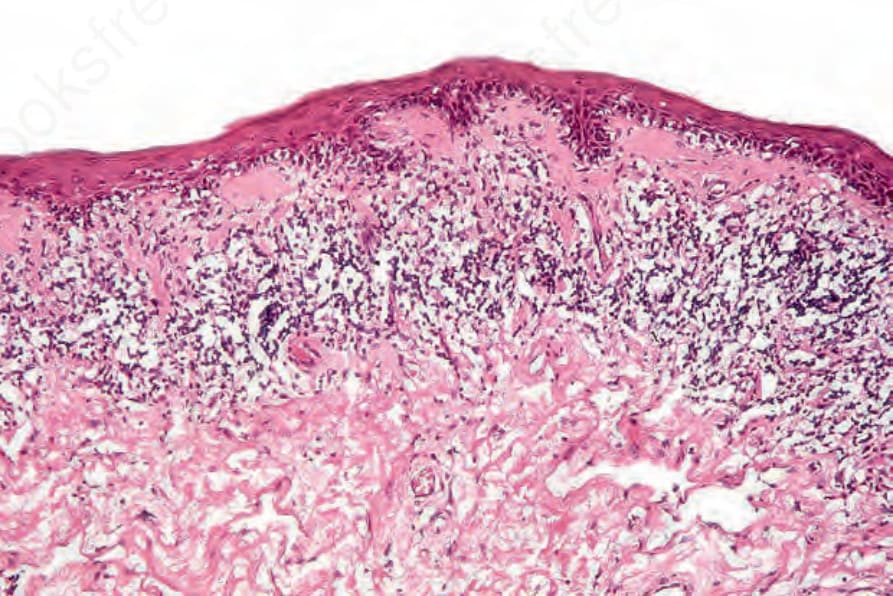
Fig. 12.58 Lichen sclerosus: early lesion showing epidermal atrophy and marked basal cell hydropic degeneration. There is a narrow zone of papillary dermal hyalinization and a bandlike infiltrate is present.
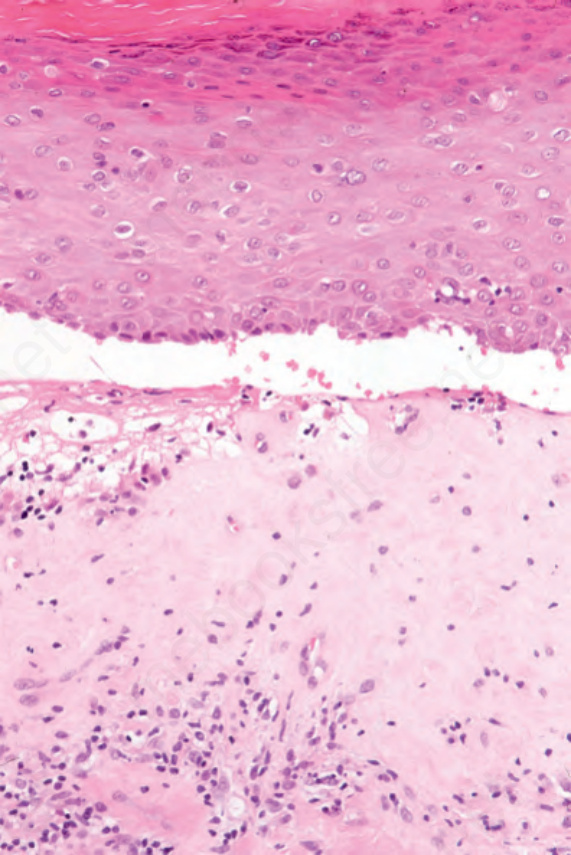
Fig. 12.62 Lichen sclerosus: occasionally, intense edema may result in subepidermal vesiculation.