Digital pacinian neuroma
Digital pacinian neuroma
Clinical features Traumatic neuroma is not a true neoplasm but instead represents a proliferative hyperplastic response to peripheral nerve injury.1,2 It may occur at any age or site, including subungual, oral cavity, penis, and rectum but is most often seen in young people, after severe accidental trauma or in older individuals following limb amputation (usually undertaken because of peripheral vascular disease), or other surgical procedures.3–13 A case after hair transplantation has been reported.14 However, trauma is not always severe and, in rare cases, a history of trauma cannot be elicited.15–17 Associations with an arteriovenous aneurysm, a human bite and multiple lesions after deep burns have been documented.18–20 Genital lesions, sometimes multiple, may be seen and are not always associated with known trauma.21 Clinically, it presents as a small firm mass, which is often painful, but is sometimes associated with local anesthesia. Multiple recurrences of cutaneous carcinoma as a result of local tumor spread along the nerves of a traumatic neuroma have been reported.22
Clinical features Digital pacinian neuroma (pacinian corpuscle hyperplasia) is a rare but distinctive type of neuroma that usually presents as a result of trauma to the fingers of adults.1–4 Lesions are small and very painful.5,6 A case has been associated with a Morton metatarsalgia.6 Erosive bone changes have been documented in one patient.7 Multiple lesions have been reported.8
Histologic features Histologically, there are numerous pacinian corpuscles intermixed with small nerve fibers and surrounded by fibrous tissue (Figs 35.296 and 35.297).
Histologic features A traumatic neuroma is characterized by a variably well-defined, but unencapsulated, mass of numerous axons and Schwann cells embedded in scar tissue adjacent to the cut end of a damaged nerve (Figs 35.294 and 35.295). The newly formed neural tissue, failing to achieve continuity with the distal portion of the affected nerve, is arranged completely haphazardly. Nuclear pleomorphism and mitotic activity are not present. Dystrophic calcification is exceptionally seen.23 Granular cell change can rarely occur in traumatic neuroma.24,25 A rare oral lesion associated with intraepithelial proliferation of axons has been documented.26
Accessory digits often show the features of a traumatic neuroma and this may be the result of partial intrauterine amputation.27
Differential diagnosis The clinical history, together with the typical histologic appearances, is usually sufficient to make a diagnosis. The presence of numerous axons
1782 Connective tissue tumors
excised from patients with Morton metatarsalgia with that of nerves from the same area excised from autopsy patients found no differences between both groups except for slightly thicker nerves in patients with the disease.11 The authors concluded that histology has no role in confirming the diagnosis, a finding that has been supported by other studies.12,13
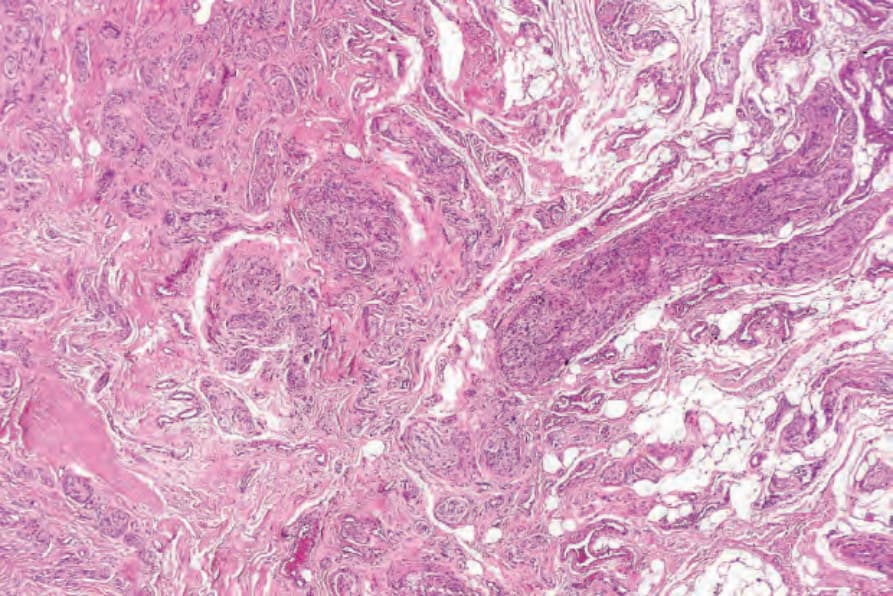
Fig. 35.294 Traumatic neuroma: arising from the cut end of this peripheral nerve is a proliferative spindle cell lesion.
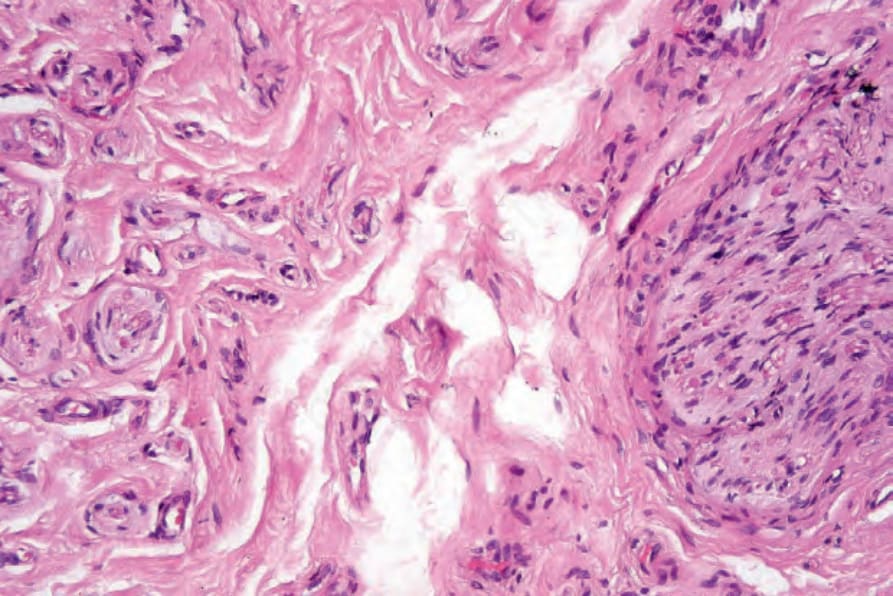
Fig. 35.295 Traumatic neuroma: high-power view.
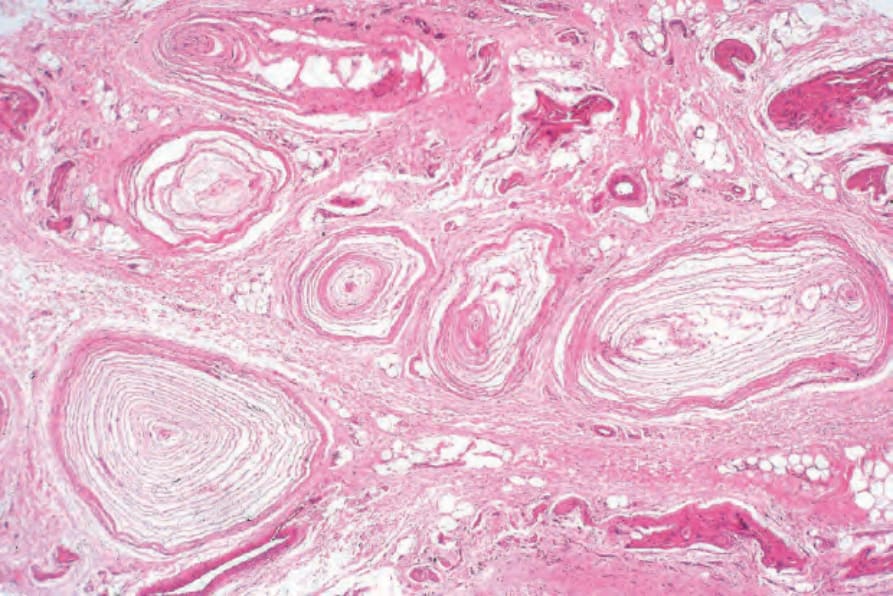
Fig. 35.296 Pacinian neuroma: this field shows an admixture of pacinian corpuscles, fibrous tissue and conspicuous nerve fibers.
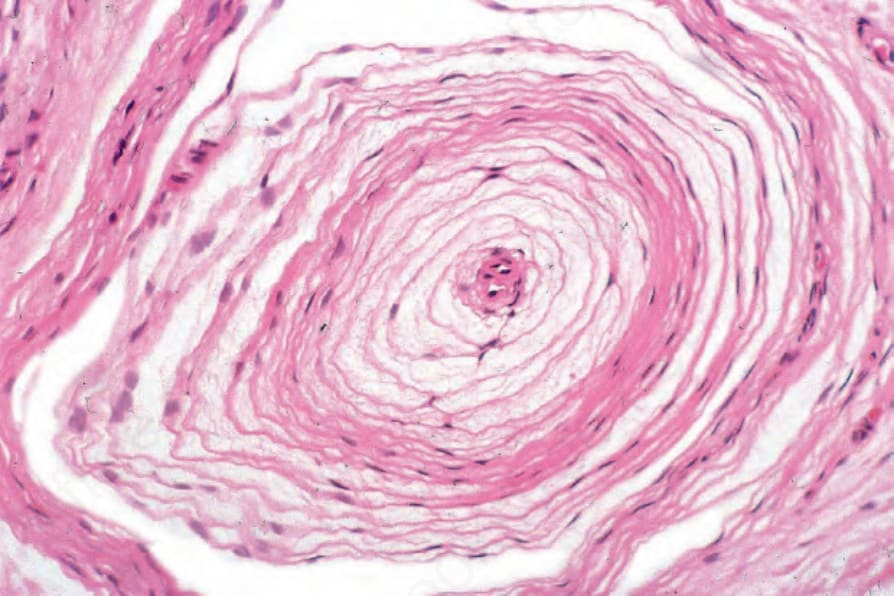
Fig. 35.297 Pacinian neuroma: high-power view showing the characteristic lamellated structure.
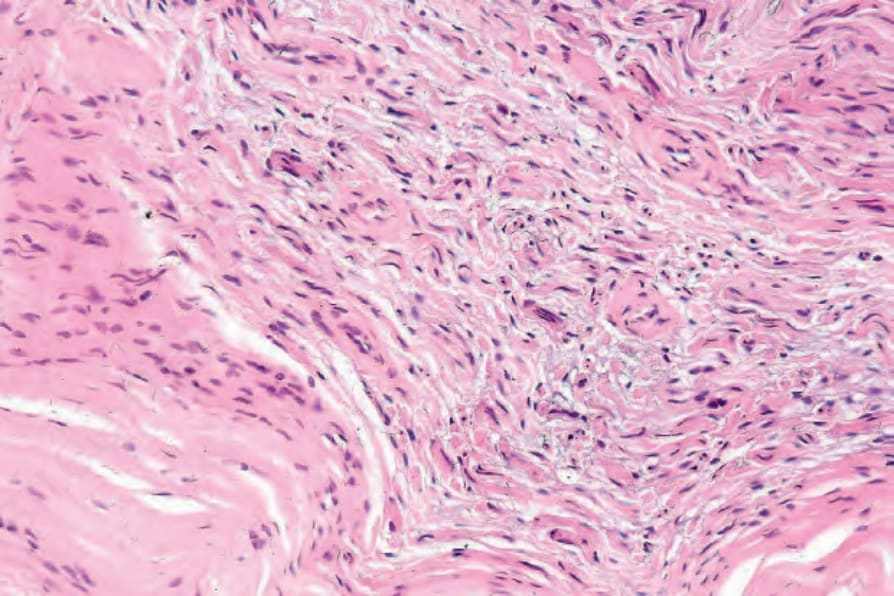
Fig. 35.299 Morton neuroma: high-power view showing numerous fibroblasts.