Hori nevus
Hori nevus
Clinical features Hori nevus (nevus fuscoceruleus zygomaticus, acquired dermal melanocytosis of the face and extremities, acquired bilateral nevus of Ota-like macules) is a rare acquired bilateral dermal melanocytosis, which predominantly affects Asian females.1–5 Patients are mostly in the third and fourth decades. Early lesions are characterized by discrete brown macules which become more confluent and slate gray in color with time.4 No spontaneous regression of the lesions is generally seen. Hori nevus shows predilection for the malar region of the cheek, followed by the forehead, upper eyelids, temples, and root/alae of the nose.3,4,6 Lesions can also develop at extrafacial locations.7,8 In males, the most common site of occurrence is forehead, and the incidence of additional extrafacial lesions is high.5 Although most commonly triggered by sun exposure and pregnancy, additional factors include
hormonal medications, stress, and trauma.4 A recent prospective study has demonstrated a positive family history in the first-degree relatives in 42% of patients.4 Hori nevus has also been reported at sites of refractory eczema and treated psoriasis.9,10 Mucosal involvement has been reported in a single patient.11
Histologic features The features are those of a superficial dermal dendritic melanocytosis. Bipolar dendritic melanocytes are dispersed throughout the upper dermis, frequently in parallel with the epidermis and in perivascular distribution.5
1295 Dermal melanocytic lesions (dermal melanocytoses)
Histologic features Common blue nevus typically lies within the deeper aspect of the reticular dermis, but occasionally may present in the superficial dermis or extend from the papillary dermis to the subcutaneous fat (Fig. 25.227). Although the overlying epidermis is usually normal, coexistent junctional activity (or a banal intradermal component) is sometimes present – the combined nevus (see above).23 There is a population of frequently heavily pigmented, bipolar, dendritic spindled cells, associated with a host-derived dense fibroblastic and collagenous spindled cell response, and commonly accompanied by heavily pigmented melanophages (Figs 25.228 and 25.229).4 Mitotic figures are rarely found, and there is no pleomorphism. The melanocytes frequently form aggregates around cutaneous appendages, blood vessels, and nerves, and are often oriented parallel to the surface epithelium. In general, the infiltrate of the common blue nevus is much denser than that of the nevi of Ito or Ota. Rare examples of smooth muscle hyperplasia within common/ combined blue nevus have been reported.24
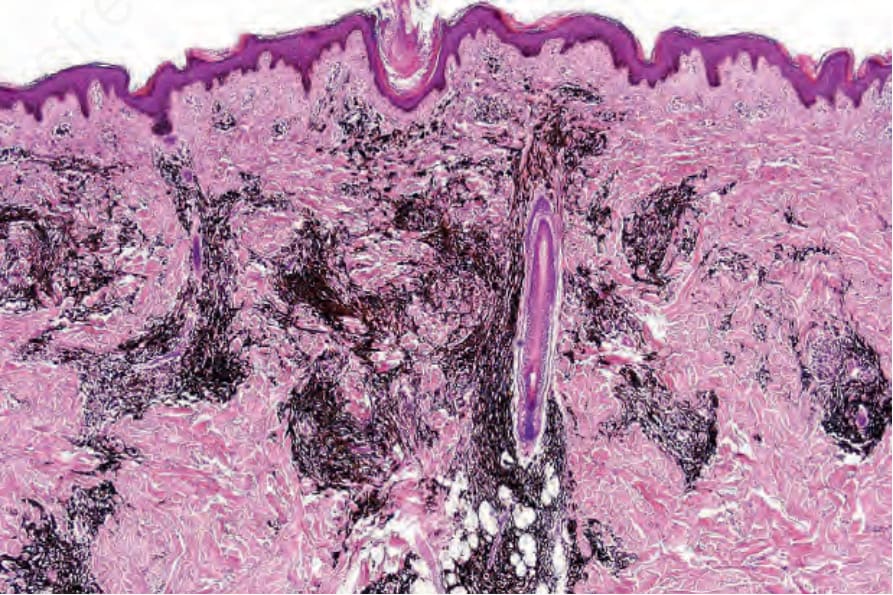
Fig. 25.227 Common blue nevus: this highly pigmented spindled cell neoplasm extensively involves the reticular dermis.
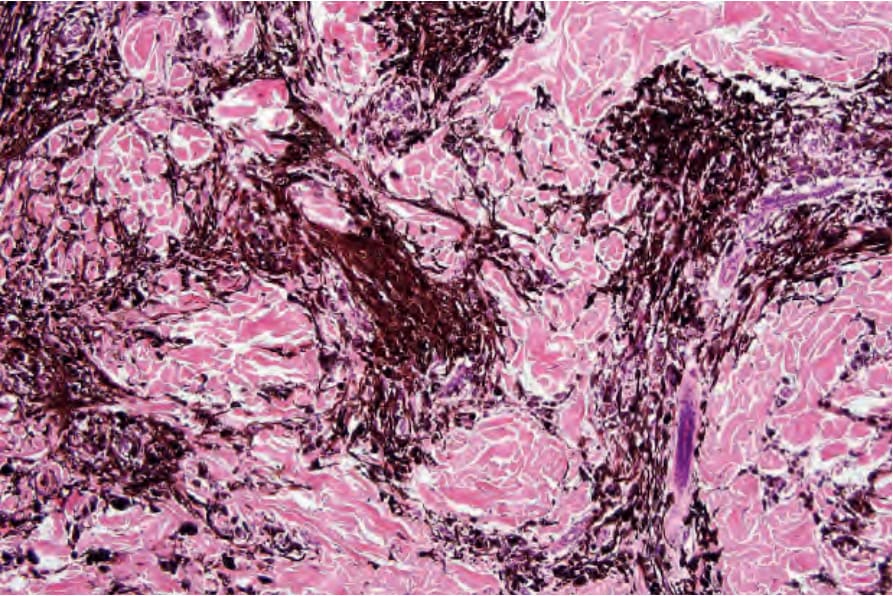
Fig. 25.228 Common blue nevus: medium-power view.