Nevus of Ota
Nevus of Ota
Clinical features Nevus of Ota (oculodermal melanosis, nevus fuscoceruleus ophthalmomaxillaris) is not uncommon in the Japanese, but is only occasionally seen in Caucasians and pigmented races. It is an ill-defined slate blue, usually
1294 Melanocytic nevi
The blue clinical appearances of nevus of Ito, the two previously mentioned lesions, and the blue nevus (see below) are artifacts due to the scattering of light during its passage through the relatively turbid dermis with absorption of all other spectral components.
Histologic features The lesion is indistinguishable from the nevus of Ota.
Histologic features The epidermis may show hyperpigmentation and increased numbers of melanocytes, but there is no junctional activity. Situated within the upper and mid-dermis are collections of heavily pigmented, spindle-shaped, bipolar, or dendritic melanocytes (Figs 25.221 and 25.222).1,3 Most are oriented parallel to the skin surface, but they may sometimes be seen encircling epidermal appendages.1 There is a minimal fibroblastic component.
Melanoma developing in the background of a nevus of Ito reported recently harbored mutations of the GNAQ and BAP1 gene.10
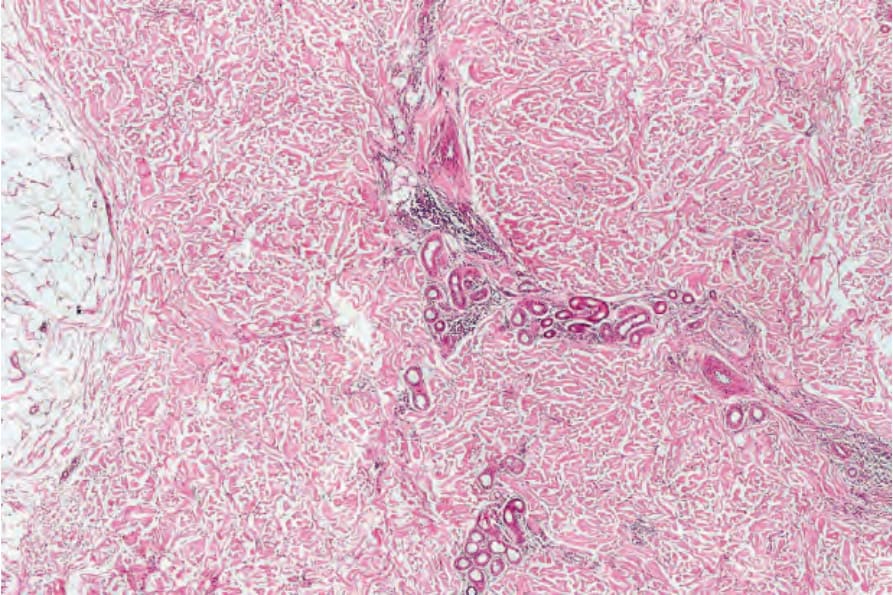
Fig. 25.218 Mongolian blue spot: at low-power examination, the features are subtle, comprising increased cellularity in the deeper dermis.
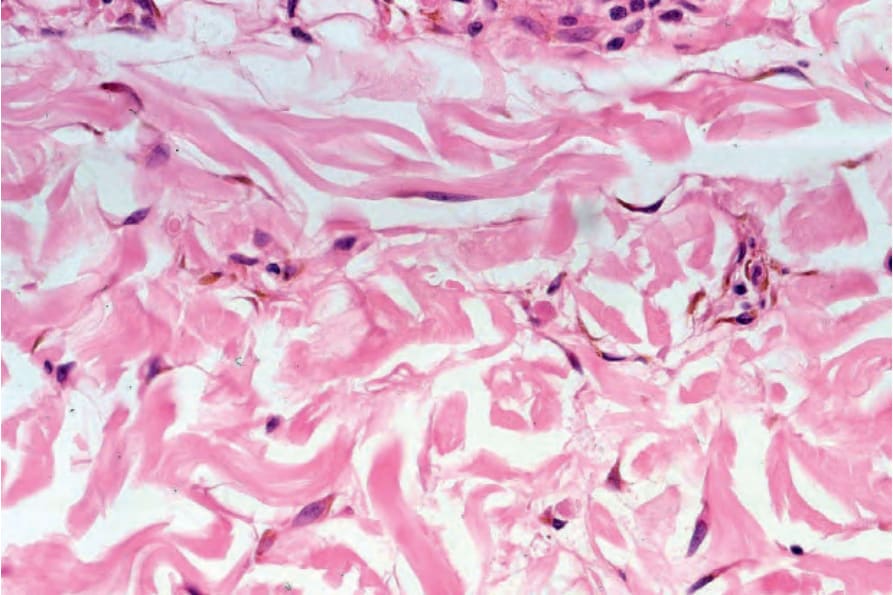
Fig. 25.219 Mongolian blue spot: scattered bipolar and dendritic cells are present.
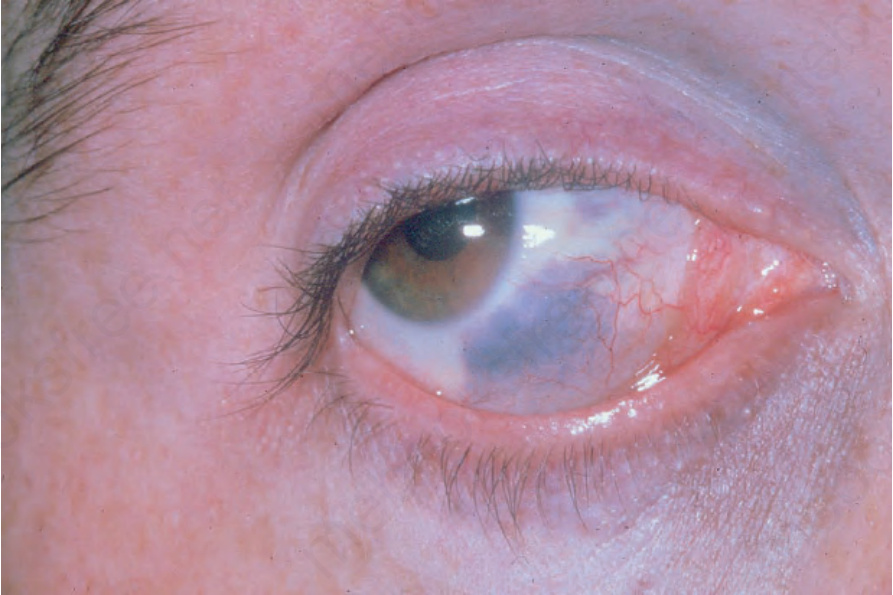
Fig. 25.220 Nevus of Ota: there is scleral involvement and a periocular bluish discoloration is evident. By courtesy of the Institute of Dermatology, London, UK.
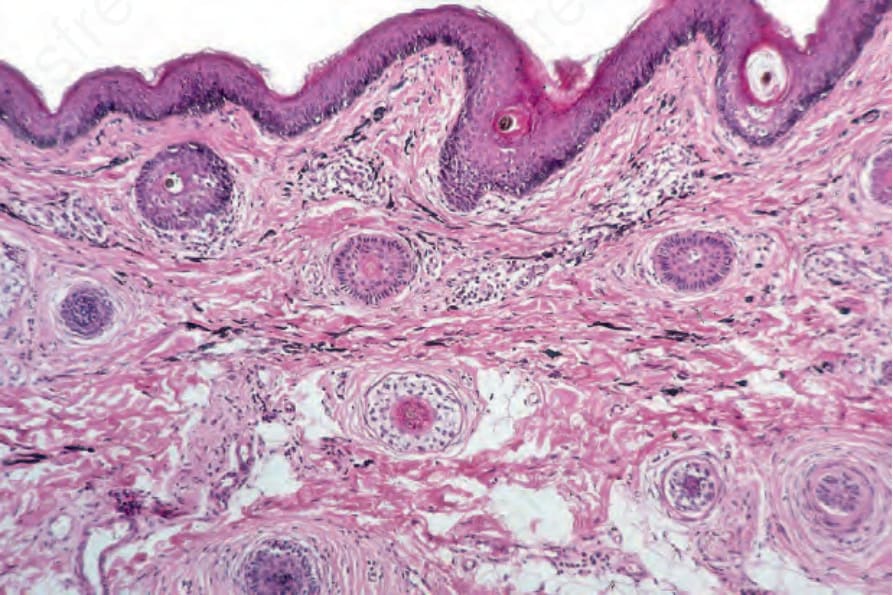
Fig. 25.221 Nevus of Ota: small numbers of bipolar and dendritic cells are present (hematoxylin and eosin and Masson-Fontana stain).
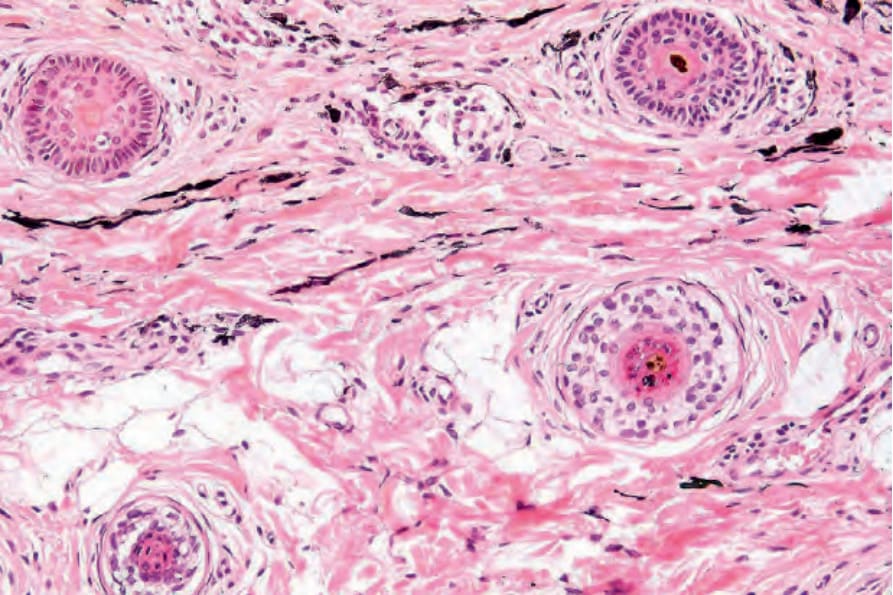
Fig. 25.222 Nevus of Ota: high-power view.
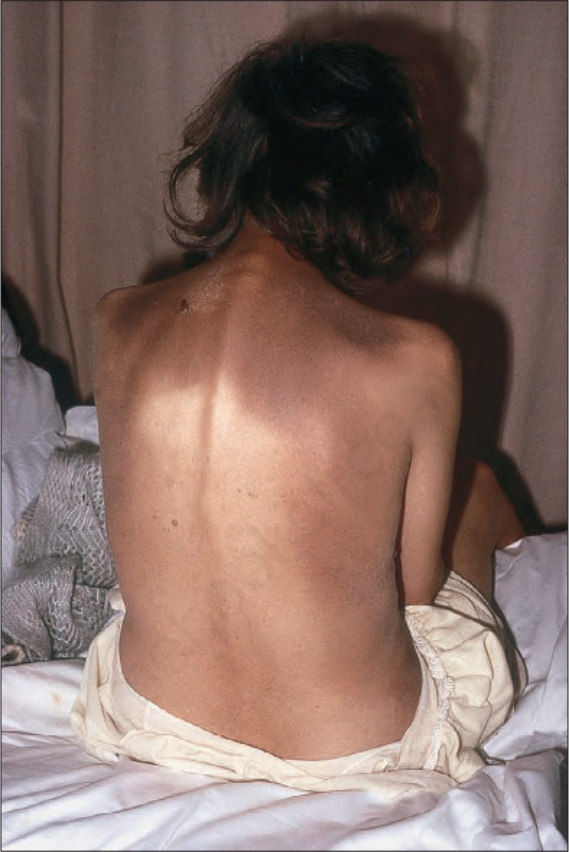
Fig. 25.223 Nevus of Ito: characteristic discoloration involving the shoulder and scapular regions. By courtesy of M.M. Black, MD, St Thomas’ Hospital, London, UK.