Protothecosis
Protothecosis
Clinical features
Protothecosis is a rare condition, representing infection by the achloric (achlorophyllic) alga Prototheca, usually P. wickerhamii.1–5 Fewer than 200 cases have been reported.6–9 Several infections with P. zopfii have also been recorded.1,5,10–12 The alga is assumed to be inoculated into the skin by minor trauma, presumably from contaminated water or soil. Prototheca are ubiquitous in nature, being found in the mucus flux of trees, water stabilization ponds, acid rivers and lakes, and a variety of animals including cows, dogs, cats, and deer.13–15 The disease has been reported worldwide.16 One recorded case occurred after an arthropod bite.14
Diseases caused by Prototheca include isolated cutaneous lesions, olecranon bursitis, and disseminated infection.1 There have been isolated reports of onychoprotothecosis and infection following corneal grafting.17,18 Protothecosis (especially in its disseminated form) occurs in iatrogenically immunosuppressed solid organ and hematopoietic stem cell transplant recipients, and in patients with diabetes mellitus or leukemia.1,6,8,10,12,14,15,19–23 It may also occur in those with AIDS.24–27 Some infections have been linked to corticosteroid usage.9,28 Protothecosis has also been recorded in a child with combined immunodeficiency.29 The condition manifests in the skin as a papular or eczematoid dermatitis, usually over an extremity.6,16,30 The dermatitis form is often extensive and scaly, hypertrophic, and resistant to therapy. Vesicular, herpetiform, pustular, plaquiform, ulcerative, granulomatous, and verrucous variants have been described (Fig. 18.257).1,4,6,15,28,31–34 Lesions may also resemble pyoderma gangrenosum, and abscess formation is sometimes encountered.6,15 Disseminated cutaneous lesions have been rarely reported.14,16,33,35 In immunocompetent patients, the infection is most often localized to the olecranon bursa following trauma.1,16 Localized tenosynovial involvement of the finger has been reported, one in an HIV-positive patient.7,24
Histologic features The localized lesions consist of necrotic centers surrounded by granulation and fibrous tissue with a few multinucleate giant cells. The algae are found in the necrotic centers.
In the dermatitis lesions, the epidermis is parakeratotic, acanthotic, and papillomatous, and there is a mixed infiltrate in the upper dermis, including occasional multinucleate giant cells (Fig. 18.258). Organisms (3–15 µm in
diameter) can be found at all levels of the epidermis and in the superficial dermis (Figs 18.259 and 18.260).3,15,16 Involvement of the deeper dermis and even the subcutis can occur. There is a polymorphous inflammatory infiltrate comprising lymphocytes, plasma cells, macrophages, histiocytic giant cells, eosinophils, and neutrophils. A prominent dermal lymphoid infiltrate may be encountered. Some cases, however, are associated with little or no inflammation.15 Infection can also involve the regional lymph nodes. Only basophilic spherical bodies are seen with H&E staining, while a silver stain or a PAS reaction reveals spore-like bodies in the epidermis and among the
924 Infectious diseases of the skin
A
B
inflammatory infiltrate. Sporangia with symmetrically arranged endospores is characteristic; these have been described as morula-like or daisy-like; these can measure up to 30 µm in diameter.6,15,24,36 Identification of the organism depends on culture characteristics. Diagnosis may also be confirmed by direct immunofluorescence or immunohistochemistry.24,37
Bursal lesions show stellate caseating necrosis surrounded by a palisade of epithelioid cells, Langhans giant cells, plasma cells, and lymphocytes.16,24 The organisms are present within the necrotic centers. Sinus tracts may be evident. There is associated fibrosis.
Differential diagnosis Prototheca are distinguished from green algae (Chlorella) by the absence of chloroplasts and from Coccidiodes immitis by its smaller size.2,15,38

Fig. 18.257 Protothecosis: numerous crusted and ulcerative lesions are present. By courtesy of the Institute of Dermatology, London, UK.
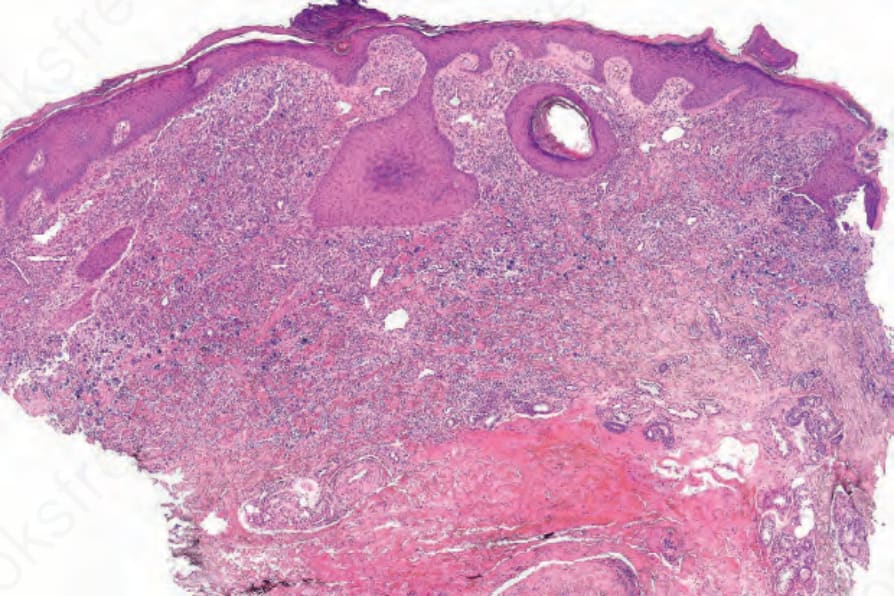
Fig. 18.258 Protothecosis: note the crusting, marked acanthosis, and heavy dermal infiltrate. By courtesy of I. Van den Berghe, AZ, Sint-Jan AV Hospital, Bruges, Belgium.
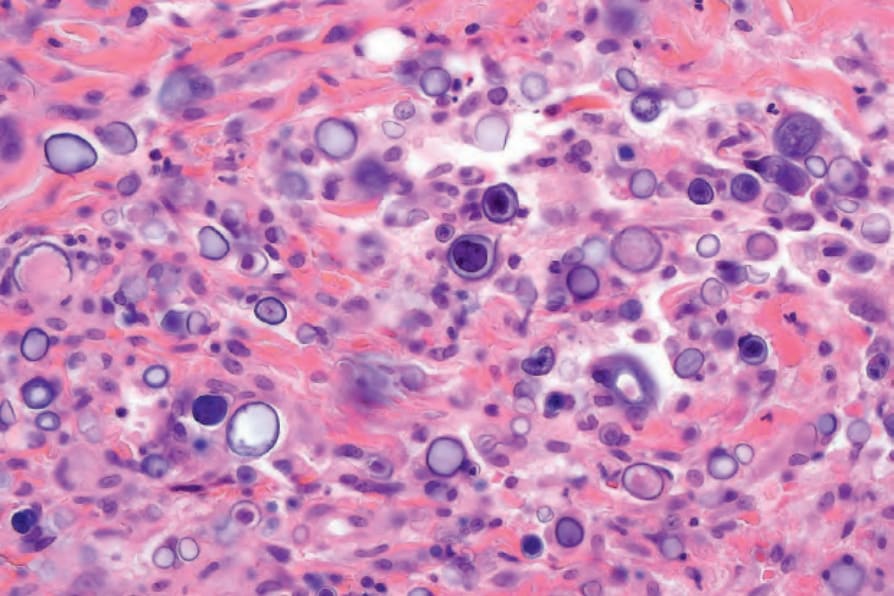
Fig. 18.259 Protothecosis: numerous organisms are present in the dermis. By courtesy of I. Van den Berghe, AZ, Sint-Jan AV Hospital, Bruges, Belgium.
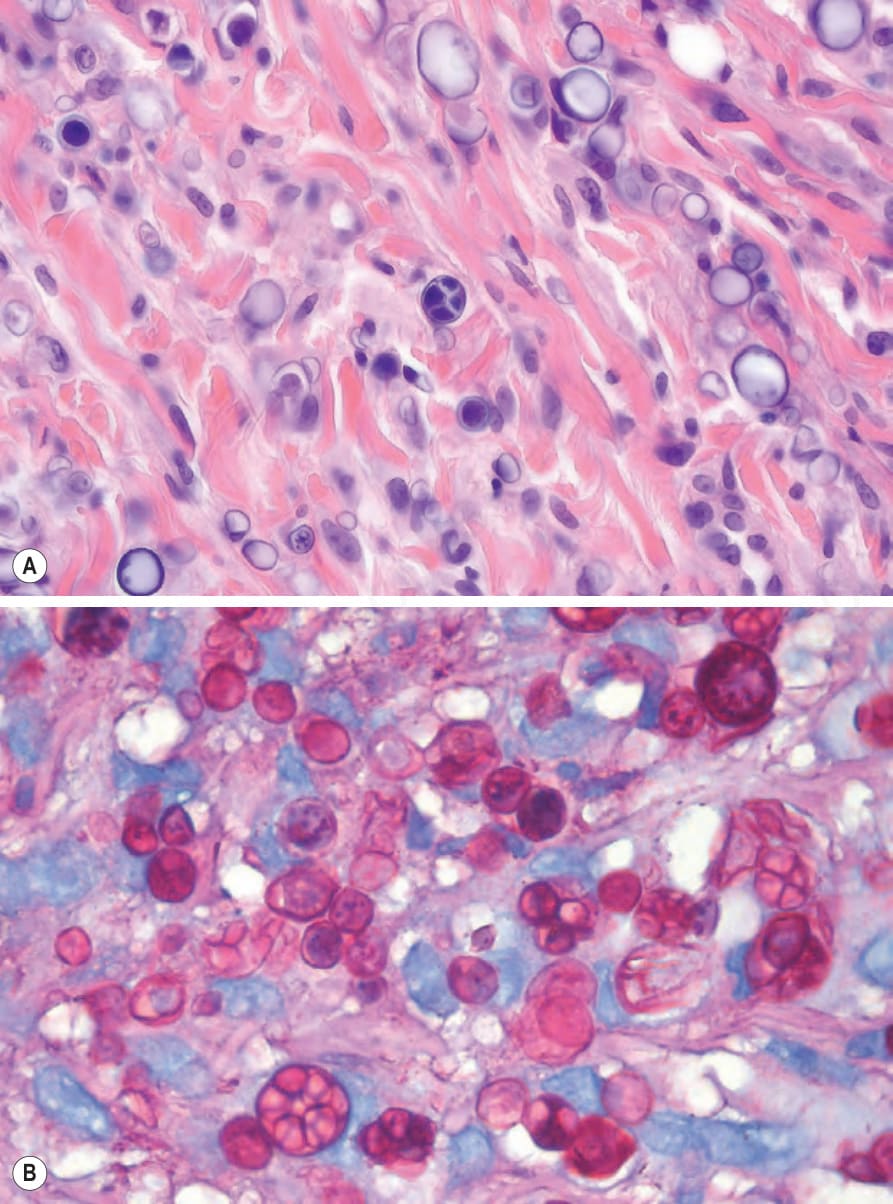
Fig. 18.260 (A, B) Protothecosis: (A) the internal septation is characteristic; (B) the organisms have thick cell walls and are PAS positive. (A) By courtesy of I. Van den Berghe, AZ, Sint-Jan AV Hospital, Bruges, Belgium; (B) By courtesy of C. Thatcher, MD, Gritzman & Thatcher Inc. Anatomical Pathologists, Johannesburg, South Africa.