Senile purpura
Senile purpura
Clinical features Senile purpura affects the extensor surfaces of the forearms, hands, and lower legs of the elderly.1,2 Corticosteroid therapy (topical or systemic) contributes to its development in some patients. Lesions are persistent, lasting 1–3 weeks, and consist of asymptomatic purpuric macules up to several centimeters in diameter, in a background of actinically damaged or atrophic skin (Fig. 16.133). Senile purpura develops because of damage to the connective tissue of the dermis, which fails to support the vasculature, rendering it more susceptible to mild trauma.
Histologic features The lesions are characterized by red cell extravasation unassociated with any significant inflammatory cell reaction. There is usually marked solar elastosis.
A
B
770 Vascular diseases
the diagnosis.6,12,13,15 Patients may also develop glomerulonephritis related to vasculitis.16,17
Laboratory studies often uncover neutropenia and ANCAs.1,2,4,5,7,8,11,13,14 Autoantibodies to human neutrophil elastase appear to be relatively specific for this condition.1
Pathogenesis and histologic features Levamisole has become a common agent used to dilute illegal cocaine, present in approximately 70% tested.17 While the precise pathogenesis is not understood, neutropenia and vasculitis/vasculopathy, including involvement of the ears, are well-known potential side effects of levamisole, thus explaining the clinical manifestations seen in cocaine users.18–21 Autoantibodies to human neutrophil elastase may also play a role.1
Histologically, biopsies may show predominantly a leukocytoclastic vasculitis, a thrombotic vasculopathy (Fig. 16.135) or a combination of both processes affecting superficial and deep dermal vessels.
Differential diagnosis The differential diagnosis includes the ANCA-vasculitides, especially polyangiitis with granulomatosis, cryoglobulinemia, and thrombotic vasculopathies, such as antiphospholipid antibody syndrome. Correlation with clinical history of cocaine use aids in distinction.
Access ExpertConsult.com for the complete list of references

Fig. 16.133 Senile purpura: trauma-induced deep purple ecchymoses on sun-damaged skin. By courtesy of J. Newton-Bishop, MD, St Thomas’ Hospital, London, UK.

Fig. 16.134 Cocaine-related retiform purpura: (A) retiform purpura with associated epidermal necrosis; (B) this patient had purpuric lesions of the ears. By courtesy of Anthony P. Fernandez, MD, PhD, Cleveland Clinic, Cleveland, USA.
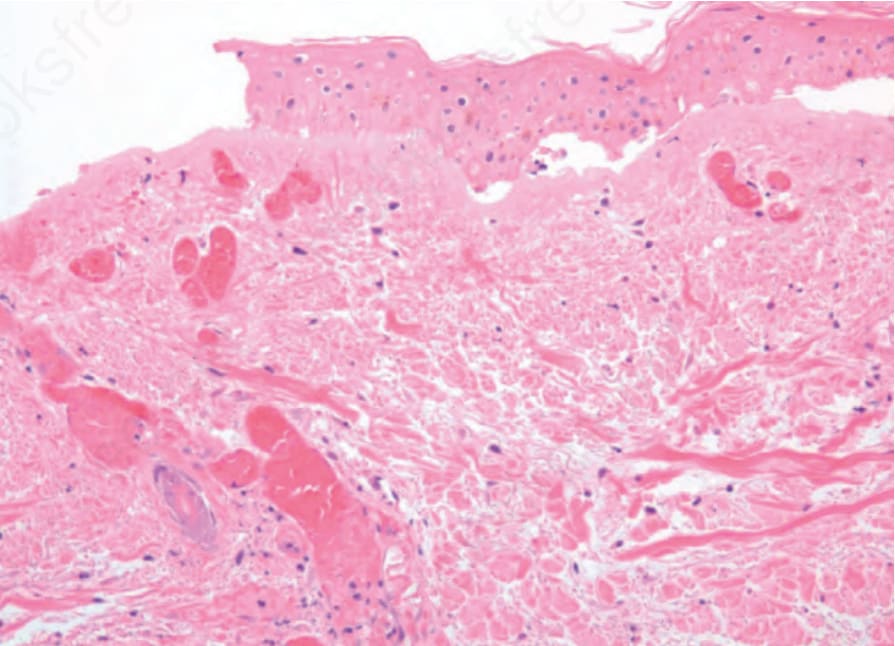
Fig. 16.135 Cocaine-related retiform purpura: in this example the biopsy demonstrated a thrombotic vasculopathy rather than leukocytoclastic vasculitis.