Vascular diseases
Vascular diseases
CHAPTER 16
for references and additional material
Introduction 714 Leukocytoclastic vasculitis 714 IgA vasculitis (Henoch-Schönlein
Thromboangiitis obliterans 747 Giant cell arteritis (temporal arteritis) 747 Juvenile temporal arteritis 750 Takayasu arteritis 750 Infection-related vasculitis 751 Paraneoplastic vasculitis 753 Vasculitis associated with palisaded
purpura) 721 Infantile acute hemorrhagic edema 723 Urticarial vasculitis 723 Granulomatosis with polyangiitis 724 Eosinophilic granulomatosis with
Disseminated intravascular coagulation 760 Cryoglobulinemia 762 Antiphospholipid antibody syndrome and
Sneddon syndrome 764 Thrombotic thrombocytopenic purpura and
hemolytic uremic syndrome 765 Immune thrombocytopenic purpura 766 Factor V (Leiden) mutation 767 Hypergammaglobulinemic purpura 767 Hyperimmunoglobulinemia D syndrome/
neutrophilic and granulomatous dermatitis 754 Lymphocytic vasculitis 754 Malignant atrophic papulosis 755 Livedoid vasculopathy and atrophie
polyangiitis 728 Microscopic polyangiitis 731 Polyarteritis nodosa 732 Kawasaki disease (mucocutaneous lymph
node syndrome) 737 Granuloma faciale 739 Erythema elevatum diutinum 741 Behçet disease 743
Mevalonate kinase deficiency 768 Superficial thrombophlebitis 768 Sclerosing lymphangitis 768 Senile purpura 769 Cocaine-related retiform purpura 769
blanche 757 Dermatological manifestations of cholesterol
crystal embolism and embolism from atrial myxoma 759
Introduction
patterns may be seen in association with a given primary vasculitis. As an example, granulomatosis with polyangiitis may be linked with either leukocytoclastic or granulomatous vasculitis.
Vasculitis and other forms of vascular damage are the subjects of this chapter. Although minimal criteria for the diagnosis of vasculitis may differ among experts, the presence of inflammation and some evidence of vascular damage in the form of vessel wall/endothelial cell necrosis or fibrinoid change fulfill most authorities’ criteria for a diagnosis of vasculitis. Some, however, apply the term less restrictively to vascular inflammation associated with non-specific histologic features, such as extravasated red cells, endothelial swelling, or karyorrhexis but without fibrinoid change or necrosis. When encountering such cases, we prefer to designate them as ‘low-grade vascular damage’ and include a comment that, although the findings may represent very early vasculitis, they do not meet strict criteria for necrotizing vasculitis. That inflammatory vascular disease is represented by a broad spectrum of histologic changes cannot be overemphasized.
The myriad schemata for the classification of the vasculitides are a reflection of the complexity of this controversial class of diseases. Over the last decade or so, several new classifications have emerged that attempt to combine both histologic and clinical information (Table 16.1).2–5 More recently, the revised Chapel Hill consensus has updated the nomenclature of vasculitidies.3 Undoubtedly, these will continue to be refined as a more complete understanding of the pathogenesis of these diseases is gained.
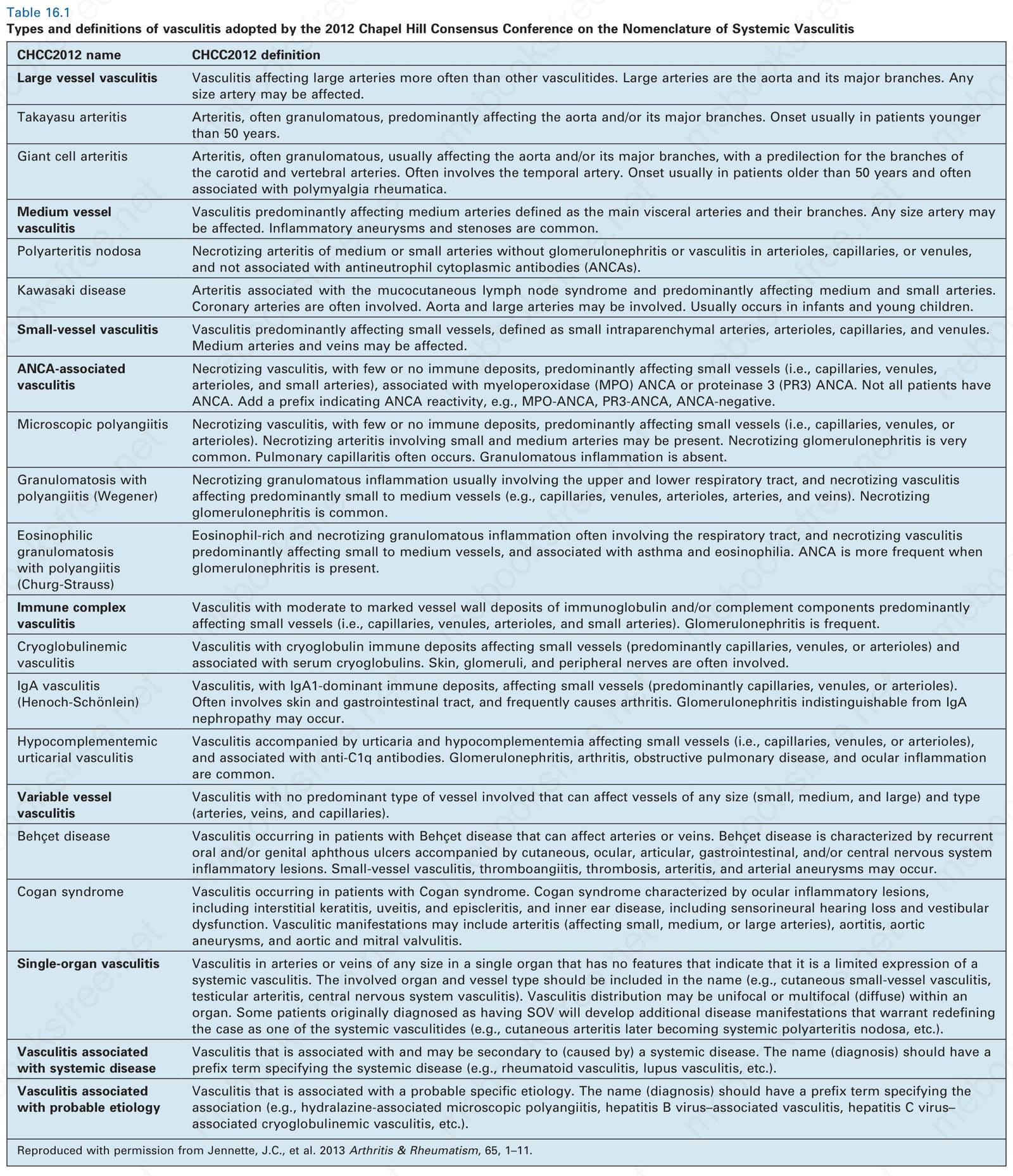
Table 16.1 Types and definitions of vasculitis adopted by the 2012 Chapel Hill Consensus Conference on the Nomenclature of Systemic Vasculitis