Psoriasis
Psoriasis
pubis or labia majora (Fig. 12.20), scrotum and perianal skin are the most common sites affected. Giant forms (of Pautrier) occur, e.g., on the scrotum, giving a pineapple appearance (Fig. 12.21).
Histologic features The histologic features are discussed in detail elsewhere, but lichenification is characterized by hyperkeratosis, hypergranulosis, uniform acanthosis, fibrosis of the papillary dermis, and an unremarkable low-grade perivascular infiltrate of mononuclear leukocytes in the superficial dermis. The papillary dermal fibrosis is streaky and perpendicular to the epidermis. Eosinophils are often present, in some cases reflecting an element of irritant contact dermatitis. At mucosal sites hyper- and orthokeratosis creates a cornified layer, resulting in the clinical appearances of white thickened plaques.
Clinical features Flexural psoriasis is the most common pattern seen in the anogenital region, with extension into the genitocrural folds and natal cleft (Figs 12.22–12.25). There are often difficulties clinically in distinguishing between psoriasis and seborrheic dermatitis. Genital and flexural disease may reflect koebnerization and is relatively common.1 In the circumcised male, the signs on the glans and distal penile shaft are similar to those of psoriasis at extragenital sites, whereas the appearances in the uncircumcised male are of balanoposthitis similar to flexural psoriasis.2 In females, well-demarcated plaques generally affect the labia majora with extension on to the mons pubis and perianal skin. Fissuring is common.3
Histologic features Histology is often unhelpful, as the changes can be non-specific. The typical features of psoriasis are rarely evident, and the presence of secondary spongiosis is common and may be misleading.
480 Diseases of the anogenital skin
Salmonella, Yersinia, and Campylobacter have also been reported preceding reactive arthritis.10–14
Sexually transmitted reactive arthritis may occur with a nongonococcal or ‘non-specific’ urethritis.7 Chlamydia trachomatis is isolated from the genitourinary tract in 40–60% of male cases; isolation is variable, however, and an indirect immunofluorescence test detects chlamydial infection in 90% of patients.15,16 Mycoplasma infection and Streptococcus viridans have also been implicated.17–19 The condition has also been linked to the acquired immunodeficiency syndrome (AIDS).20–22 Rare associations include Cyclospora, Cryptosporidium, intravesical bacillus Calmette–Guérin (BCG) immunotherapy, Gardnerella vaginalis, hepatitis B immunization, and systemic interferon-alpha (IFN-α) treatment.23–28
Reactive arthritis is more likely to occur in predisposed individuals. HLA-B27, which is thought to occur in up to 90% of patients, increases the risk of developing reactive arthritis by 25 times; the disease is also more severe in HLA-B27-positive individuals.4,29 HLA-B27 in patients with reactive arthritis correlates with ankylosing spondylitis.4 Reactive arthritis develops in 20% of HLA-B27-positive individuals after a specific infective episode.30 An association with HLA-B51 has been reported.31 Rarely, familial instances have been documented.30 Therefore, it appears that the disease is triggered in genetically predisposed individuals by an unknown mechanism precipitated by infection.
The genitourinary tract is virtually always involved in the form of urethritis, prostatitis, seminal vesiculitis, and hemorrhagic cystitis. Urethral strictures also sometimes occur and females may develop cervicitis.
Bilateral mucopurulent conjunctivitis is the usual form of eye involvement occurring in up to 35% of patients, but occasionally iritis, iridocyclitis, keratitis, or blindness occurs.32
Weight-bearing joints and the larger ones (knees, ankles, feet, and wrists) are involved by the arthritis, often together with sacroiliitis. Radiological changes include osteoporosis, erosions and loss of joint space, with multiple joints usually affected.4,30 Periostitis often affects the metatarsals, the phalanges of the feet, and the tarsal bones; occasionally, ankylosis develops in the small bones of the hands and feet. Ankylosing spondylitis, which is an important manifestation, correlates with a high erythrocyte sedimentation rate (ESR).30
In the initial stages of the arthritis the clinical picture resembles that of an acute joint infection, settling to subacute involvement. Although the arthritis in reactive arthritis usually recovers completely, chronic manifestations can sometimes occur; it is important to remember that arthritis may be the only symptom in recurrent episodes.
Skin lesions in reactive arthritis may be similar to those of psoriasis. Cutaneous manifestations include hyperkeratotic cobblestone lesions on the palms and soles and occasionally affecting the trunk and extremities (Fig. 12.26). The lesions initially present as erythematous macules; over the course of several days these become hyperkeratotic waxy papules, with an erythematous halo covered by dry hyperkeratotic material. The papules are numerous and eventually coalesce to form thickened horny plaques. Pustular lesions of the palms and soles may also be evident (keratoderma blenorrhagicum) (Fig. 12.27).
Circinate balanitis, presenting as a moist superficial erosion, 2–4 mm across, may affect the glans penis and meatus (Figs 12.28–12.30). Superficial ulceration of the oral mucosa may also occur, together with reddening and a granular appearance of the surrounding mucous membrane.4,5

Fig. 12.20 Lichen simplex of the vulva – marked lichenification of the labia majora.

Fig. 12.21 Lichen simplex chronicus. Scrotum. Giant ‘pineapple’ lesion. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.

Fig. 12.22 Psoriasis: note the symmetrical, intensely erythematous eruption involving the groins, vulva and perineum. Scaling is typically absent in flexural disease. The sharply demarcated border is characteristic. By courtesy of the Institute of Dermatology, London, UK.
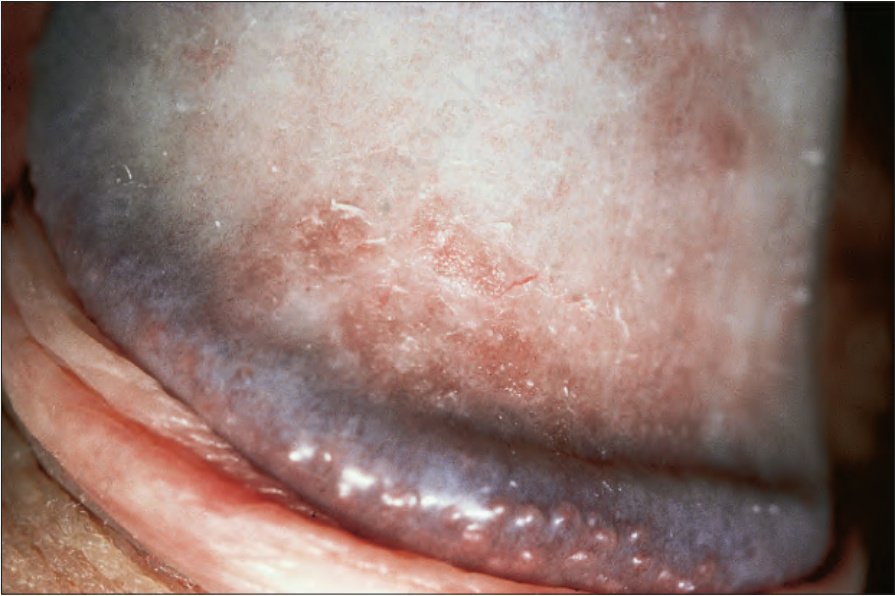
Fig. 12.24 Psoriasis: in this example a slight scale is apparent. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.25 Psoriasis: note the erythematous and slightly scaly plaque affecting the perineum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.26 Reactive arthritis: there are bilateral keratotic papules and plaques affecting the soles of the feet. By courtesy of R.A. Marsden, MD, St George’s Hospital, London, UK.
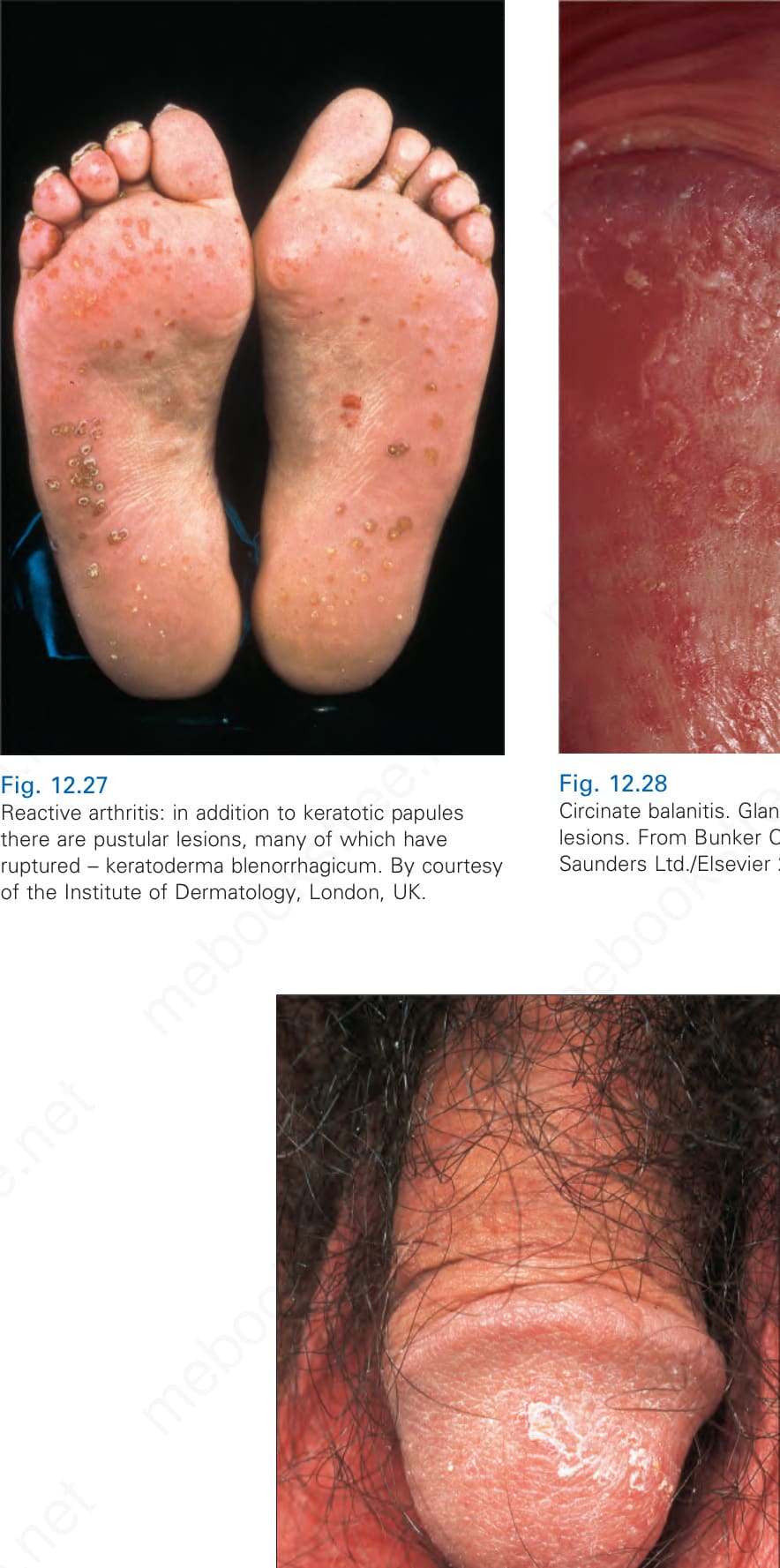
Fig. 12.27 Reactive arthritis: in addition to keratotic papules there are pustular lesions, many of which have ruptured – keratoderma blenorrhagicum. By courtesy of the Institute of Dermatology, London, UK.

Fig. 12.28 Circinate balanitis. Glans penis. Psoriasiform lesions. From Bunker C. Male Genital Skin Disease. Saunders Ltd./Elsevier 2004.