疾病定義與分類
- 疱疹樣皮膚炎(Dermatitis herpetiformis,Duhring-Brocq disease)為廣泛、強烈 pruritic 的 papulovesicular eruption。與 celiac disease 高度相關,視為 celiac disease 的皮膚外表現。
- 各年齡皆可,好發第二至第四個十年,男女比 2:1,兒童較少見(芬蘭兒童年發生率 0.56/10 萬,約成人的六分之一)。盛行率以北歐最高(芬蘭達 75.3/10 萬),白人為主,亞洲與黑人罕見。家族聚集常見(可能 autosomal dominant,達 10.5%)。
臨床表現與病程(Clinical course)
- 病灶可對稱,主要成群分布於後頭皮、肩、背、臀及四肢伸側。因強烈搔抓,常以 excoriation/lichenification 為主,完整水皰罕見;偶見似 bullous pemphigoid 的較大水皰。口腔受累罕見。
- 少見表現:palmoplantar purpura 局限於掌蹠而背側倖免(兒童較多);petechiae 偶限於指尖。
- 與 celiac disease 關係:65–75% 病人有 celiac disease(gluten-sensitive enteropathy, GSE)的組織學證據,但僅約 20% 有 malabsorption 臨床表現(多輕微);推測所有 DH 病人皆有不同程度 GSE。
- 關聯:antigastric parietal cell antibody(10–25%)、gastric hypochlorhydria(50–90%)、gastric atrophy(50–70%)、antithyroid 抗體與甲狀腺疾病、insulin-dependent diabetes mellitus、結締組織疾病(SLE、Sjögren syndrome);腸道 lymphoma 風險增加。暴露於 iodine 可誘發或加重。
治療
- 對 dapsone(50–200 mg/day)反應顯著,常用於診斷與治療目的;數小時內緩解 pruritus,續而皮疹清除;停藥後 2–3 天皮疹回復。疾病持續多年、通常終身。Gluten-free diet 可使部分病人長期緩解或降低每日 dapsone 需求。
致病機轉(Pathogenesis)
- 與 celiac disease 同樣有高 HLA 關聯:HLA-B8(80–90%)、HLA-DR3(90–95%)、HLA-DQ2(95–100%);目前認為顯著正關聯在 class II 抗原 DQ2。缺乏 HLA-DQ2/DQ8 haplotype 有高陰性預測值。
- 所有 DH 病人在 perilesional skin 的 dermal papillae 有顆粒狀 IgA 沉積(許多並有 in vivo-bound fibrin);可見 granular linear 或 fibrillar pattern。其他免疫球蛋白通常無,但 C3 常見(形成膜攻擊複合體 C5–C9,致 neutrophil 趨化與表皮下水皰)。Dapsone 治療後皮膚 IgA 沉積仍可偵測,長期 gluten-free diet 後有時消失。
- 抗體:endomysial 抗體(達 70%,高度專一)反應 tissue transglutaminase(tTG);epidermal transglutaminase 抗體更常見且似為最敏感血清標記。腸道為 TG2、皮膚為 TG3,兩者交叉反應或抗原漂移可能解釋黏膜與皮膚表現。循環 IgA anti-tTG 抗體為 DH 與 celiac disease 的特徵性表現。
- IgA 在皮膚「固定」後經替代途徑活化補體 → 釋放 neutrophil 趨化因子 → dermal papillary edema、fibrin 沉積與水皰;可能也涉及細胞媒介免疫(γ/δ T cells)。
組織病理特徵(Histopathology)
- 組織學標誌:dermal papillary neutrophilic microabscess,在早期紅斑病灶或遠離水皰處最易見(有時需檢視多層次切片才找到)。
- 膿瘍演變始於 dermal papillae 尖端的 fibrin 與 polymorphs,伴 collagen 退化與水腫;發展為 subepidermal microvesicles,續為 multilocular subepidermal blisters。
- 水皰腔含水腫液、網狀 fibrin 與大量 polymorphs;與 bullous pemphigoid 不同,水皰底部通常呈 dermal papillary outline 消失(effacement)。
- 真皮混合浸潤含 lymphocytes、histiocytes、豐富 neutrophils,特徵性 leukocytoclasis(nuclear dust);血管內皮腫脹但無血管炎。Eosinophils 偶多但多為 neutrophils 後 24–48 小時才出現。偶見 acantholysis(造成混淆)。
- Jejunal biopsy:villous blunting、crypt elongation、表面上皮細胞扁平與微絨毛喪失、intraepithelial γ/δ lymphocytic 浸潤,程度從 partial 至 subtotal villous atrophy;去除 gluten 後可回復正常。
鑑別診斷
- Neutrophil 為主的 subepidermal 水皰伴 dermal papillary microabscesses,除 DH 外也可見於 vesicular pemphigoid、bullous systemic lupus erythematosus、inflammatory epidermolysis bullosa、linear IgA disease;區分依賴臨床資訊與免疫螢光(見 Table 4.6)。
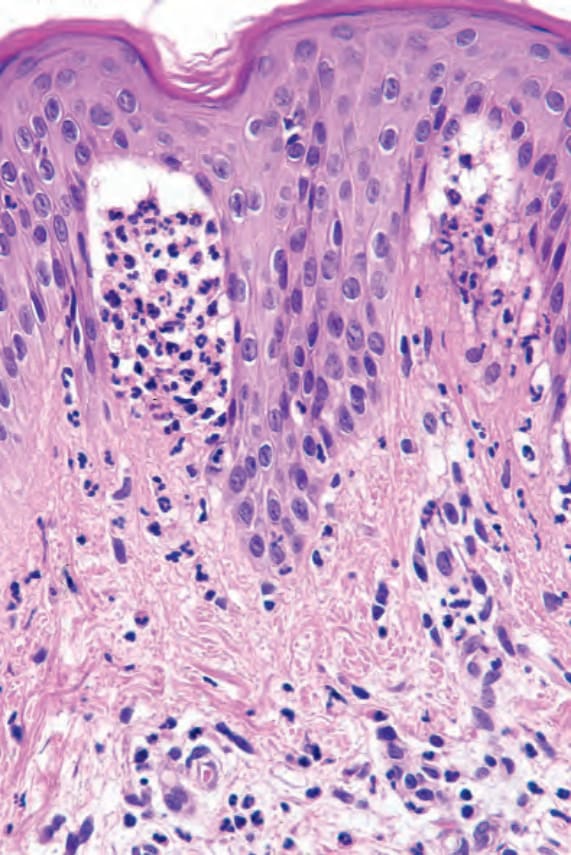
圖 4-137:Dermatitis herpetiformis,早期病灶顯示明顯 neutrophil 微膿瘍。
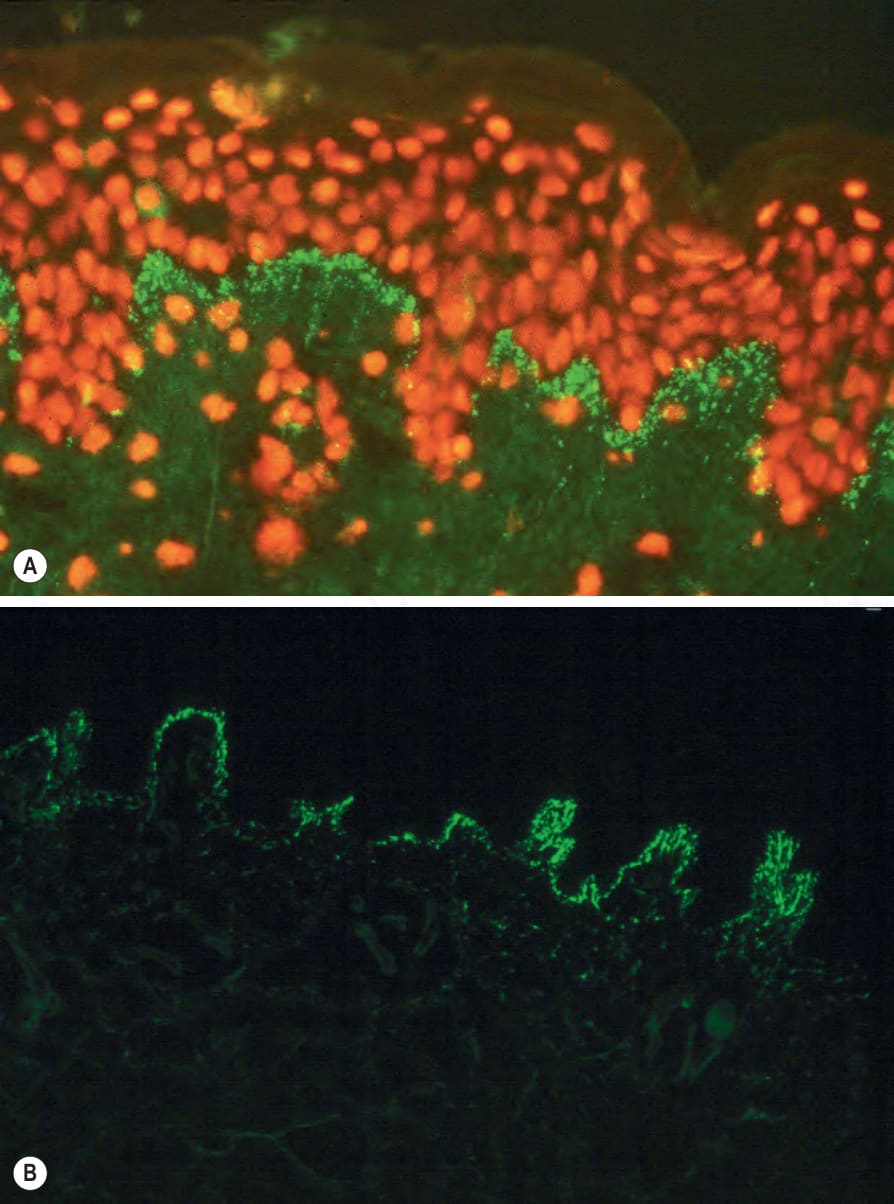
圖 4-136:Dermatitis herpetiformis,直接免疫螢光顯示 dermal papillae 內顆粒狀 IgA 沉積與 fibrin 沉積。